

Percutaneous fractionated radiotherapy of the groin to eliminate lymphatic fistulas after vascular surgery
- PMID: 36755343
- PMCID: PMC9909919
- DOI: 10.1186/s40001-023-01033-6
Percutaneous fractionated radiotherapy of the groin to eliminate lymphatic fistulas after vascular surgery
Abstract
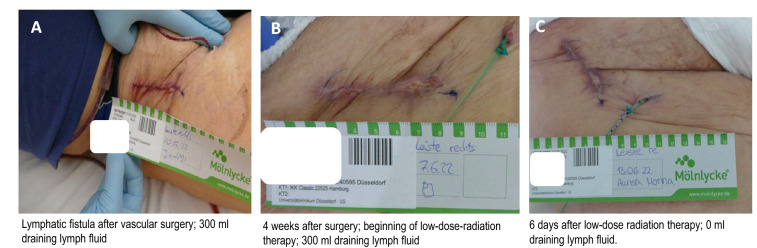
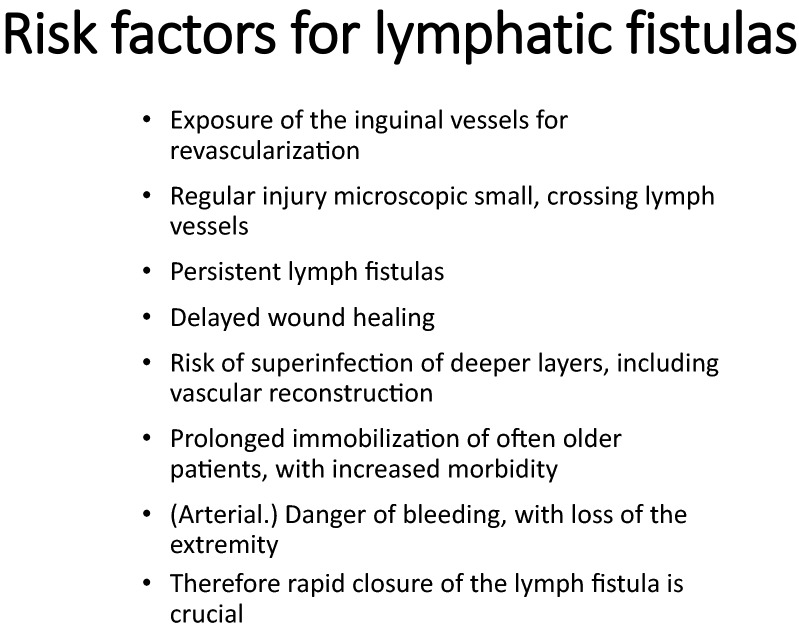
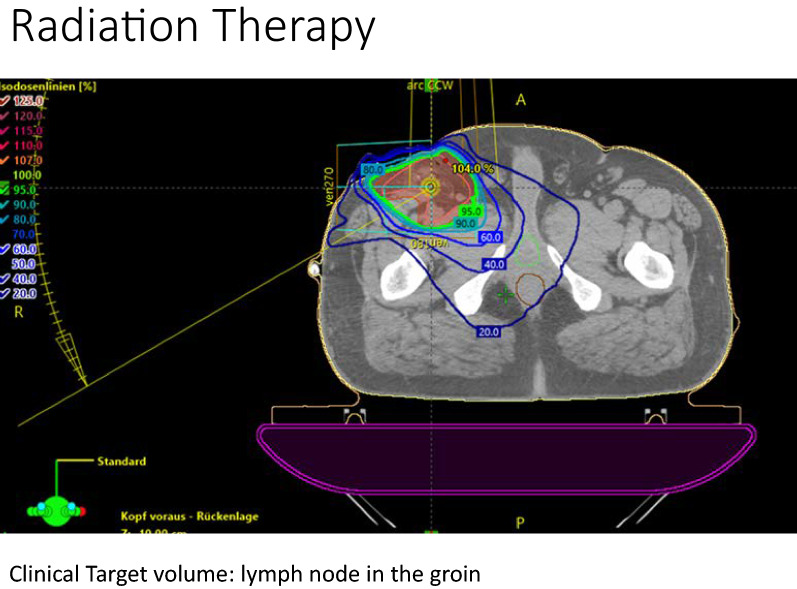
Background: Vascular surgery of the inguinal area can be complicated by persistent lymphatic fistulas. Rapid and effective treatment is essential to prevent infection, sepsis, bleeding, and possible leg amputation. Current data on irradiation of lymphatic fistulas lack recommendation on the appropriate individual and total dose, the time of irradiation, and the target volume. Presumably, a dose of 0.3-0.5 to 1-12 Gy should be sufficient for the purpose. Currently, radiotherapy is a "can" recommendation, with a level 4 low evidence and a grade C recommendation, according to the DEGRO S2 guidelines. As part of a pilot study, we analyzed the impact and limitations of low-dose radiation therapy in the treatment of inguinal lymphatic fistulas.
Patients and methods: As a part of an internal quality control project, patients with lymphatic fistulas irradiated in the groin area after vascular surgery for arterial occlusive disease (AOD) III-IV, repair of pseudo aneurysm or lymph node dissection due to melanoma were selected, and an exploratory analysis on retrospectively collected data performed.
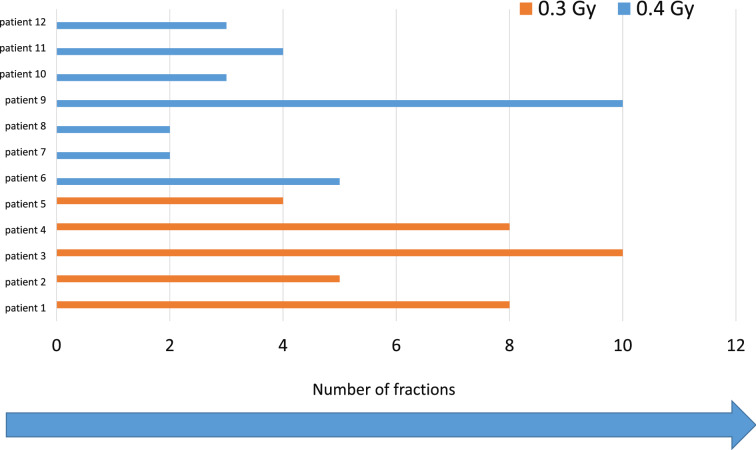
Results: Twelve patients (10 males and 2 females) aged 62.83 ± 12.14 years underwent open vascular reconstruction for stage II (n = 2), III (n = 1), and IV (n = 7) arterial occlusive disease (AOD), lymph node dissection for melanoma (n = 1) or repair of a pseudoaneurysm (n = 1). Surgical vascular access was obtained through the groin and was associated with a persistent lymphatic fistula, secreting more than 50 ml/day. Patients were irradiated five times a week up to a maximum of 10 fractions for the duration of the radiation period. Fraction of 0.4 Gy was applied in the first 7 cases, while 5 patients were treated with a de-escalating dose of 0.3 Gy. There was a resolution of the lymphatic fistula in every patient without higher grade complications.
Conclusion: Low-dose irradiation of the groin is a treatment option for persistent lymphatic fistula after inguinal vascular surgery.
Keywords: Amputation; Benign disease; Radiation therapy; Side effects; Surgery; Wound healing.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
