

Clinical Outcome of Endoscopic Procedure in Patients with Shunt Malfunction
- PMID: 36755510
- PMCID: PMC10009242
- DOI: 10.3340/jkns.2022.0089
Clinical Outcome of Endoscopic Procedure in Patients with Shunt Malfunction
Abstract
Objective: The goal of this study was to analyze the clinical outcomes of endoscopic third ventriculostomy (ETV) and endoscopic septostomy when shunt malfunction occurs in a patient who has previously undergone placement of a ventriculoperitoneal shunt.
Methods: From 2001 to 2020 at Seoul National University Children's Hospital, patients who underwent ETV or endoscopic septostomy for shunt malfunction were retrospectively analyzed. Initial diagnosis (etiology of hydrocephalus), age at first shunt insertion, age at endoscopic procedure, magnetic resonance or computed tomography image, subsequent shunting data, and follow-up period were included.
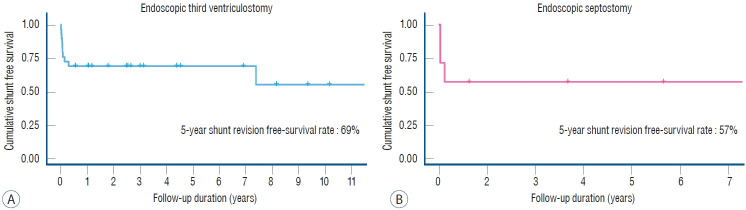
Results: Thirty-six patients were included in this retrospective study. Twenty-nine patients, 18 males and 11 females, with shunt malfunction underwent ETV. At the time of shunting, the age ranged from 1 day to 15.4 years (mean, 2.4 years). The mean age at the time of ETV was 13.1 years (range, 0.7 to 29.6 years). Nineteen patients remained shunt revision free. The 5-year shunt revisionfree survival rate was 69% (95% confidence interval [CI], 0.54-0.88). Seven patients, three males and four females, with shunt malfunction underwent endoscopic septostomy. At the time of shunting, the age ranged from 0.2 to 12 years (mean, 3.9 years). The mean age at the time of endoscopic septostomy was 11.9 years (range, 0.5 to 29.5 years). Four patients remained free of shunt revision or addition. The 5-year shunt revision-free survival rate was 57% (95% CI, 0.3-1.0). There were no complications associated with the endoscopic procedures.
Conclusion: The results of our study demonstrate that ETV or endoscopic septostomy can be effective and safe in patients with shunt malfunction.
Keywords: Endoscopy; Hydrocephalus; Shunt failure; Ventriculoperitoneal shunt; Ventriculostomy.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Endoscopic third ventriculostomy: an outcome analysis of primary cases and procedures performed after ventriculoperitoneal shunt malfunction.J Neurosurg. 2005 Nov;103(5 Suppl):393-400. doi: 10.3171/ped.2005.103.5.0393. J Neurosurg. 2005. PMID: 16302610
-
Endoscopic Third Ventriculostomy Instead of Shunt Revision in Children Younger Than 3 Years of Age.World Neurosurg. 2016 Apr;88:92-96. doi: 10.1016/j.wneu.2015.12.047. Epub 2015 Dec 28. World Neurosurg. 2016. PMID: 26732961 Clinical Trial.
-
Complications of endoscopic third ventriculostomy in previously shunted patients.Neurosurgery. 2008 Jul;63(1 Suppl 1):ONS168-74; discussion ONS174-5. doi: 10.1227/01.neu.0000335032.31144.17. Neurosurgery. 2008. PMID: 18728596
-
Role of Secondary Endoscopic Third Ventriculostomy in Children: Review of an Institutional Experience.Pediatr Neurosurg. 2019;54(3):188-195. doi: 10.1159/000500641. Epub 2019 Jun 3. Pediatr Neurosurg. 2019. PMID: 31158842 Review.
-
Third ventriculostomy in shunt malfunction.World Neurosurg. 2013 Feb;79(2 Suppl):S22.e21-6. doi: 10.1016/j.wneu.2012.02.005. Epub 2012 Feb 10. World Neurosurg. 2013. PMID: 22381847 Review.
Cited by
-
Successful endoscopic third ventriculostomy in a patient with 40 years of ventriculoperitoneal shunt dependency since infancy: a case report.Childs Nerv Syst. 2024 Dec 18;41(1):60. doi: 10.1007/s00381-024-06724-x. Childs Nerv Syst. 2024. PMID: 39692859
References
-
- Albanese V, Tomasello F, Sampaolo S. Multiloculated hydrocephalus in infants. Neurosurgery. 1981;8:641–646. - PubMed
-
- Aldana PR, Kestle JR, Brockmeyer DL, Walker ML. Results of endoscopic septal fenestration in the treatment of isolated ventricular hydrocephalus. Pediatr Neurosurg. 2003;38:286–294. - PubMed
-
- Baldauf J, Fritsch MJ, Oertel J, Gaab MR, Schröder H. Value of endoscopic third ventriculostomy instead of shunt revision. Minim Invasive Neurosurg. 2010;53:159–163. - PubMed
-
- Baskin JJ, Manwaring KH, Rekate HL. Ventricular shunt removal: the ultimate treatment of the slit ventricle syndrome. J Neurosurg. 1998;88:478–484. - PubMed
-
- Bilginer B, Oguz KK, Akalan N. Endoscopic third ventriculostomy for malfunction in previously shunted infants. Childs Nerv Syst. 2009;25:683–688. - PubMed
LinkOut - more resources
Full Text Sources
