

Collaboration between local nephrologists and the transplant centre ensures good outcomes in post-transplant care
- PMID: 36755830
- PMCID: PMC9900581
- DOI: 10.1093/ckj/sfac232
Collaboration between local nephrologists and the transplant centre ensures good outcomes in post-transplant care
Abstract
Background: Despite substantial improvements in short-term kidney allograft survival, median long-term survival remains at a standstill. It is unclear whether and to what extent a transplant centre's post-transplant care influences long-term outcomes.
Methods: We retrospectively analysed 501 single kidney transplant recipients (KTRs) who underwent transplantation between 2009 and 2018 and did not develop rejection or de novo donor-specific antibodies (dnDSA) within the first post-transplant year. After that, KTRs were either followed exclusively every 3 months by the transplant centre (n = 197) or every 3 months by local nephrologists (n = 304) with only yearly follow-up by the transplant centre. We analysed kidney allograft outcomes regarding estimated glomerular filtration rate (eGFR) decline, proteinuria, development of dnDSA and rejection.
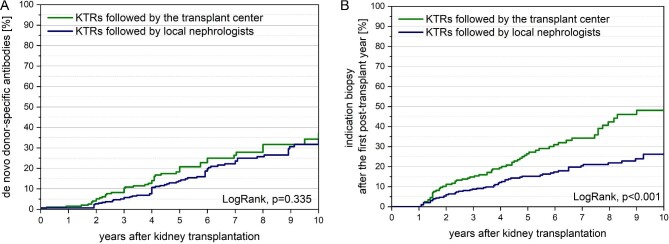
Results: No differences between the two groups were observed in the baseline characteristics and the characteristics at the end of the first post-transplant year (P > .05). KTRs followed by local nephrologists were comparable to KTRs followed by the transplant centre concerning patient survival (P = .541), kidney allograft survival (P = .385), eGFR decline (P = .488), progression of proteinuria (P > .05), the development of dnDSA (P = .335) and T-cell-mediated rejection (P = .480). KTRs followed by the transplant centre were more likely to undergo indication biopsies in case of allograft dysfunction and dnDSA (P < .001). Antibody-mediated rejection was diagnosed earlier and more frequently (P = .059), recurrent glomerulonephritis was diagnosed earlier and more frequently (P = .026) and immunosuppression was modified earlier and more frequently in response to histological findings (P = .038).
Conclusions: Our findings suggest that close collaboration between local nephrologists and the transplant centre ensures good allograft outcomes independent of the caregiver. Greater biopsy activity in the transplant centre allows for earlier diagnosis of allograft dysfunction as the basis for novel treatment options.
Keywords: ABMR; donor-specific antibodies; eGFR decline; kidney transplantation; proteinuria.
© The Author(s) 2022. Published by Oxford University Press on behalf of the ERA.
Figures





References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
