

Hair regrowth treatment efficacy and resistance in androgenetic alopecia: A systematic review and continuous Bayesian network meta-analysis
- PMID: 36755885
- PMCID: PMC9900126
- DOI: 10.3389/fmed.2022.998623
Hair regrowth treatment efficacy and resistance in androgenetic alopecia: A systematic review and continuous Bayesian network meta-analysis
Abstract
Background: Androgenetic alopecia (AGA) affects almost half the population, and several treatments intending to regenerate a normal scalp hair phenotype are used. This is the first study comparing treatment efficacy response and resistance using standardized continuous outcomes.
Objective: To systematically compare the relative efficacy of treatments used for terminal hair (TH) regrowth in women and men with AGA.
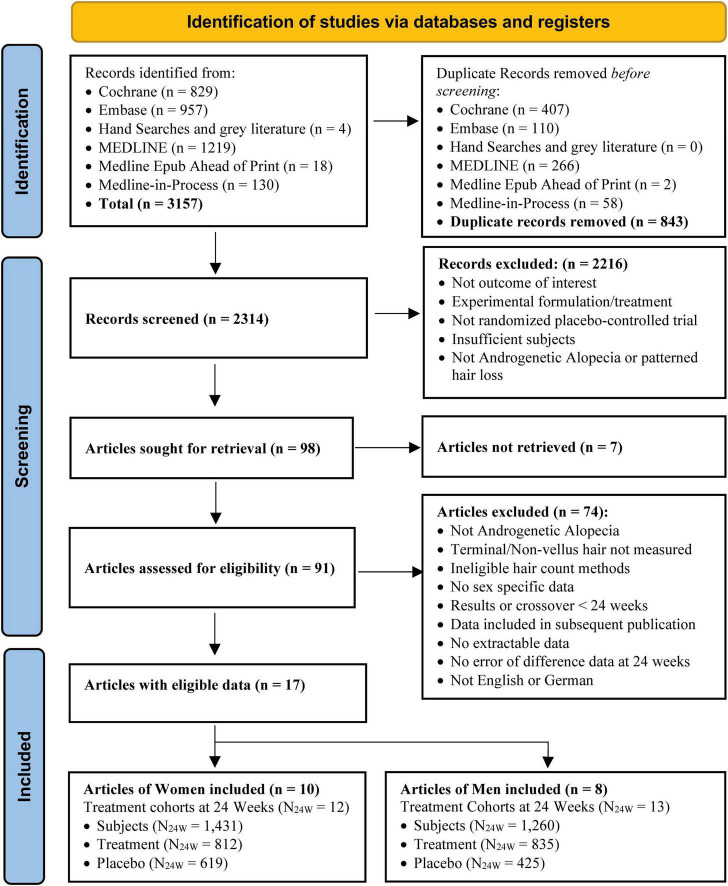
Methods: A systematic literature review was conducted (from inception to August 11, 2021) to identify randomized, Placebo-controlled trials with ≥ 20 patients and reporting changes in TH density after 24 weeks. Efficacy was analyzed by sex at 12 and 24 weeks using Bayesian network meta-analysis (B-NMA) and compared to frequentist and continuous outcomes profiles.
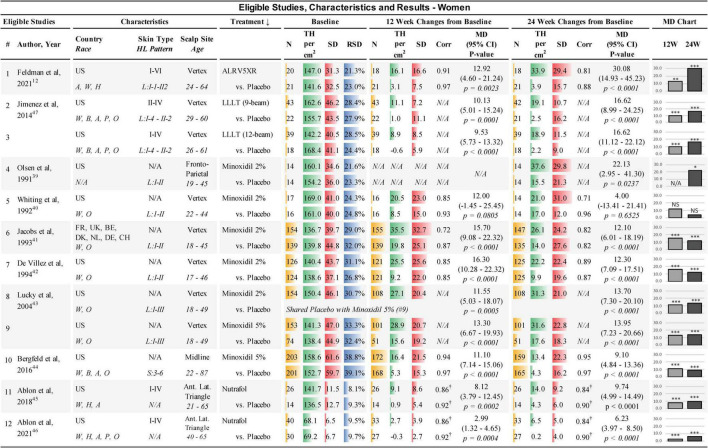
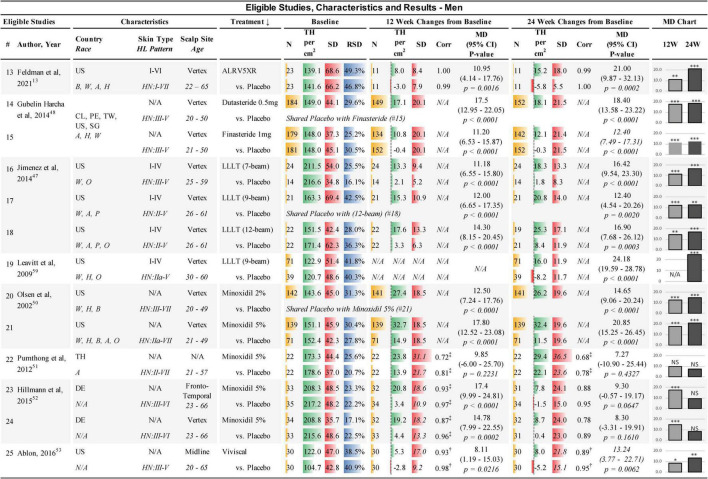
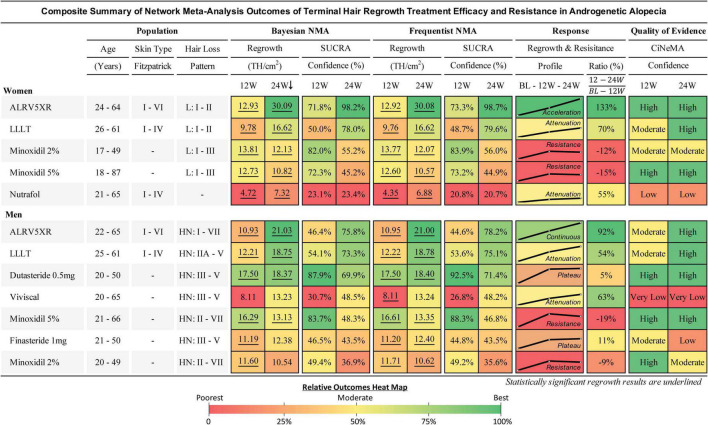
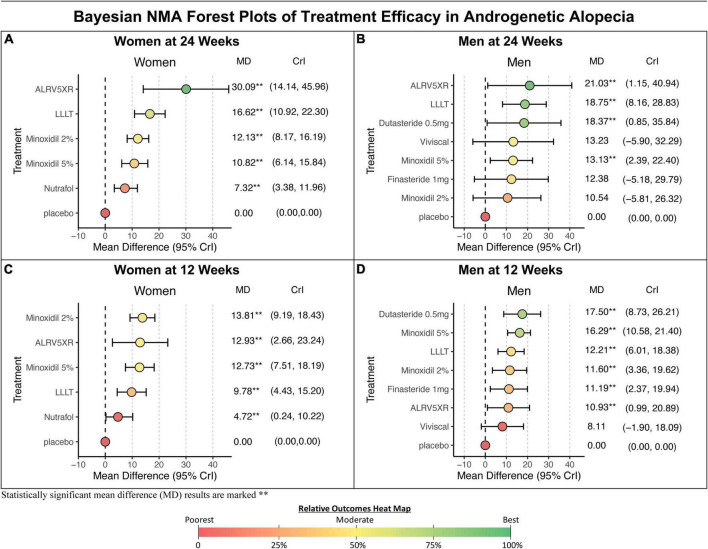
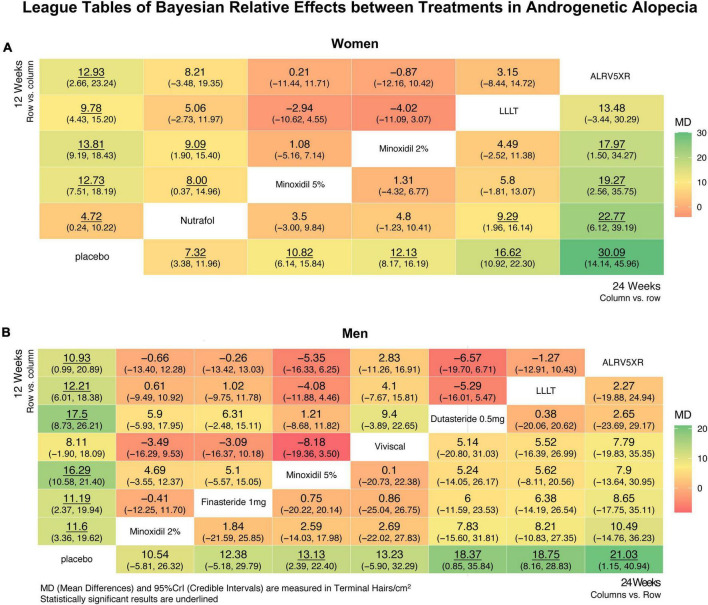
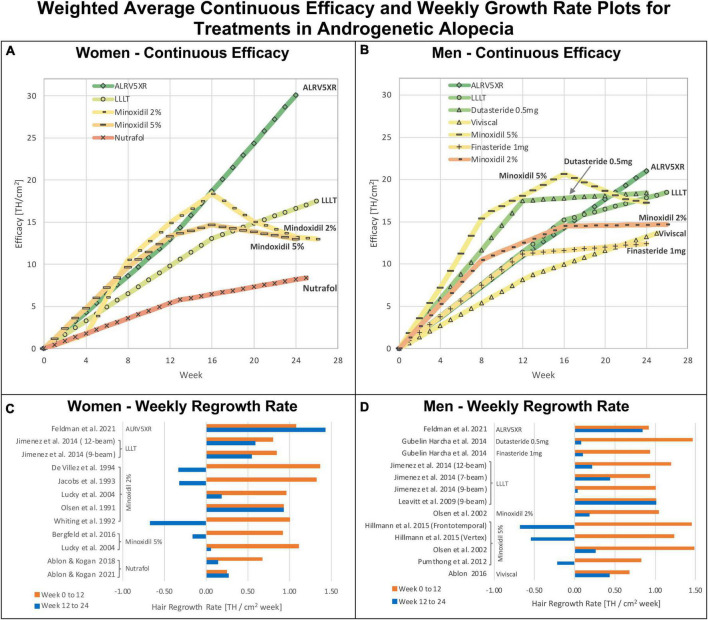
Results: The search identified 2,314 unique articles. Ninety-eight were included for full-text review, and 17 articles met the inclusion criteria for data extraction and analyses. Eligible treatments included ALRV5XR, Dutasteride 0.5 mg/day, Finasteride 1 mg/day, low-level laser comb treatment (LLLT), Minoxidil 2% and 5%, Nutrafol, and Viviscal. At 24 weeks, the B-NMA regrowth efficacy in TH/cm2 and significance (**) in women were ALRV5XR: 30.09**, LLLT: 16.62**, Minoxidil 2%: 12.13**, Minoxidil 5%: 10.82**, and Nutrafol: 7.32**, and in men; ALRV5XR: 21.03**, LLLT: 18.75**, Dutasteride: 18.37**, Viviscal: 13.23, Minoxidil 5%: 13.13**, Finasteride: 12.38, and Minoxidil 2%: 10.54. Two distinct TH regrowth response profiles were found; Continuous: ALRV5XR regrowth rates were linear in men and accelerated in women; Resistant: after 12 weeks, LLLT, Nutrafol, and Viviscal regrowth rates attenuated while Dutasteride and Finasteride plateaued; Minoxidil 2% and 5% lost some regrowth. There were no statistical differences for the same treatment between women and men. B-NMA provided more accurate, statistically relevant, and conservative results than the frequentist-NMA.
Conclusion: Some TH regrowth can be expected from most AGA treatments with less variability in women than men. Responses to drug treatments were rapid, showing strong early efficacy followed by the greatest resistance effects from flatlining to loss of regrowth after 12-16 weeks. Finasteride, Minoxidil 2% and Viviscal in men were not statistically different from Placebo. LLLT appeared more efficacious than pharmaceuticals. The natural product formulation ALRV5XR showed better efficacy in all tested parameters without signs of treatment resistance (see Graphical abstract).
Systematic review registration: www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42021268040, identifier CRD42021268040.
Keywords: ALRV5XR; Dutasteride; Finasteride; LLLT; Minoxidil; Nutrafol; Viviscal; hair loss.
Copyright © 2023 Feldman, Gentile, Piwko, Motswaledi, Gorun, Pesachov, Markel, Silver, Brenkel, Feldman, Kamen, Uleryk, Guevara-Aguirre and Fiebig.
Conflict of interest statement
Arbor Life Labs (ALL) is the owner of ALRV5XR. PRF was employed by ALL. SG, JP, MM, MIS, MB, OJF, CLK, JG-A, EU, and KMF received honoraria from ALL. CP was employed by CHP Pharma Inc. EU was employed by Uleryk Consulting. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- McMichael A, Hordinsky M. Hair and scalp disorders: medical, surgical, and cosmetic treatments. 2nd ed. Boca Raton, FL: CRC Press; (2018). 10.1201/9781351169844 - DOI
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous