

A Systematic Review and Meta-analysis of the Impact of Radiation-Related Lymphopenia on Outcomes in High-Grade Gliomas
- PMID: 36756098
- PMCID: PMC9902102
- DOI: 10.1055/s-0042-1753504
A Systematic Review and Meta-analysis of the Impact of Radiation-Related Lymphopenia on Outcomes in High-Grade Gliomas
Abstract
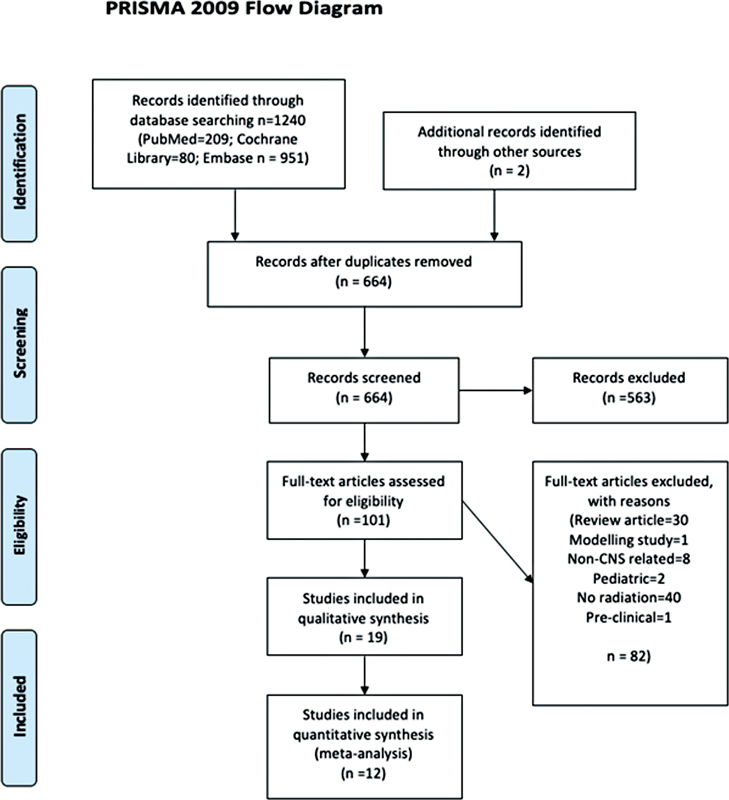
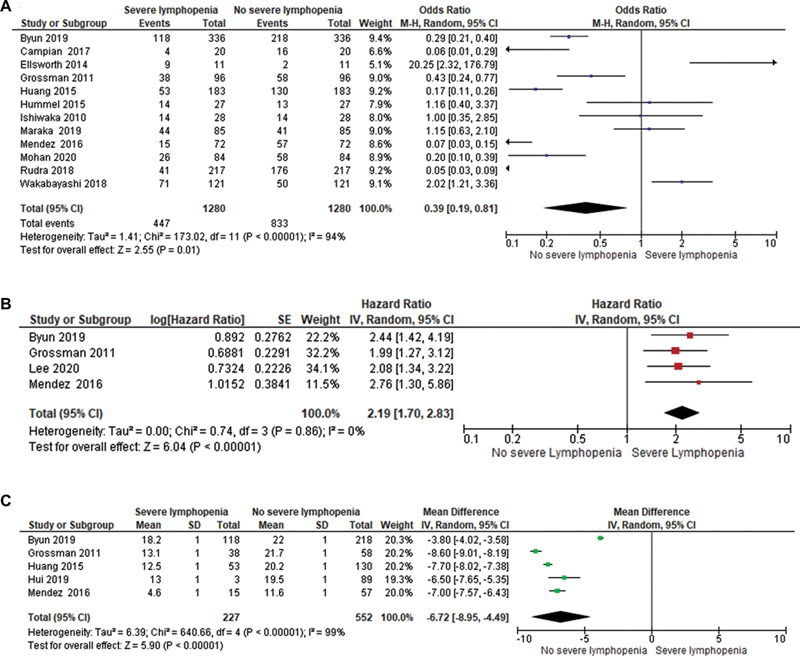
Supriya MallickIntroduction Malignant gliomas are the most common primary malignant brain tumors and are typically treated with maximal safe surgical resection followed by chemoradiation. One of the unintended effects of radiation is depletion of circulating lymphocyte pool, which has been correlated with inferior overall survival outcomes. Methods A comprehensive and systematic searches of the PubMed, Cochrane Central, and Embase databases were done to assess the studies that have reported radiation-related lymphopenia in high-grade gliomas. Hazard ratios (HRs), odds ratios (OR), and mean differences were represented with Forest plots comparing patients with severe lymphopenia and no severe lymphopenia. Review Manager Version 5.3 (The Nordic Cochrane Centre, Copenhagen, Denmark) was used for the analysis. Results Nineteen studies were included in the final systematic review and 12 studies were included in the meta-analysis. The odds of developing severe lymphopenia were 0.39 (95% CI:0.19, 0.81, I 2 = 94%, p = 0.01). Patients with severe lymphopenia were at increased risk of death with a pooled HR = 2.19 (95% CI: 1.70, 2.83, I 2 = 0%, p <0.00001) compared to patients with no severe lymphopenia. The mean difference in survival between patients with severe lymphopenia and no severe lymphopenia was -6.72 months (95% CI: -8.95, -4.49, I 2 = 99%, p <0.00001), with a better mean survival in the no severe lymphopenia group. Conclusion Radiation-induced severe lymphopenia was associated with poor overall survival and increased risk of death. Photon therapy, larger planning target volume, higher brain dose, higher hypothalamus dose, and female gender were associated with increased risk of severe lymphopenia.
Keywords: high-grade gliomas; lymphopenia; radiation; systematic review.
MedIntel Services Pvt Ltd. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. ( https://creativecommons.org/licenses/by-nc-nd/4.0/ ).
Conflict of interest statement
Conflict of Interest None declared. A.A.S. served on advisory boards for Novocure in 2019.
Figures

Similar articles
-
A systematic review and meta-analysis of the impact of radiation-related lymphopenia on outcomes in pancreatic cancer.Future Oncol. 2022 May;18(15):1885-1895. doi: 10.2217/fon-2021-0483. Epub 2022 Feb 8. Future Oncol. 2022. PMID: 35132868
-
Prognostic Value and Risk Factors of Treatment-Related Lymphopenia in Malignant Glioma Patients Treated With Chemoradiotherapy: A Systematic Review and Meta-Analysis.Front Neurol. 2022 Jan 4;12:726561. doi: 10.3389/fneur.2021.726561. eCollection 2021. Front Neurol. 2022. PMID: 35058869 Free PMC article.
-
A Systematic Review of Radiation-Related Lymphopenia in Genito-urinary Malignancies.Cancer Invest. 2021 Oct;39(9):769-776. doi: 10.1080/07357907.2021.1960992. Epub 2021 Aug 17. Cancer Invest. 2021. PMID: 34313522
-
Survival in Patients With Severe Lymphopenia Following Treatment With Radiation and Chemotherapy for Newly Diagnosed Solid Tumors.J Natl Compr Canc Netw. 2015 Oct;13(10):1225-31. doi: 10.6004/jnccn.2015.0151. J Natl Compr Canc Netw. 2015. PMID: 26483062 Free PMC article.
-
Impact of radiotherapy parameters on the risk of lymphopenia in urological tumors: A systematic review of the literature.Radiother Oncol. 2022 May;170:64-69. doi: 10.1016/j.radonc.2022.02.030. Epub 2022 Mar 4. Radiother Oncol. 2022. PMID: 35257847
Cited by
-
Impact of intensity-modulated proton therapy in reducing radiation-induced lymphopenia in glioma patients.Neurooncol Adv. 2024 Jun 4;6(1):vdae088. doi: 10.1093/noajnl/vdae088. eCollection 2024 Jan-Dec. Neurooncol Adv. 2024. PMID: 39045310 Free PMC article.
-
The need for paradigm shift: prognostic significance and implications of standard therapy-related systemic immunosuppression in glioblastoma for immunotherapy and oncolytic virotherapy.Front Immunol. 2024 Feb 8;15:1326757. doi: 10.3389/fimmu.2024.1326757. eCollection 2024. Front Immunol. 2024. PMID: 38390330 Free PMC article. Review.
-
How proton therapy fits into the management of adult intracranial tumors.Neuro Oncol. 2024 Mar 4;26(12 Suppl 2):S26-S45. doi: 10.1093/neuonc/noad183. Neuro Oncol. 2024. PMID: 38437667 Free PMC article. Review.
References
-
- Omuro A, DeAngelis L M. Glioblastoma and other malignant gliomas: a clinical review. JAMA. 2013;310(17):1842–1850. - PubMed
-
- European Organisation for Research and Treatment of Cancer Brain Tumor and Radiotherapy Groups ; National Cancer Institute of Canada Clinical Trials Group . Stupp R, Mason W P, van den Bent M J. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352(10):987–996. - PubMed
-
- European Organisation for Research and Treatment of Cancer Brain Tumour and Radiation Oncology Groups ; National Cancer Institute of Canada Clinical Trials Group . Stupp R, Hegi M E, Mason W P. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009;10(05):459–466. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources