

Identification of biomarkers to stratify response to B-cell-targeted therapies in systemic lupus erythematosus: an exploratory analysis of a randomised controlled trial
- PMID: 36756239
- PMCID: PMC9894756
- DOI: 10.1016/S2665-9913(22)00332-0
Identification of biomarkers to stratify response to B-cell-targeted therapies in systemic lupus erythematosus: an exploratory analysis of a randomised controlled trial
Abstract
Background: Systemic lupus erythematosus (SLE) is a complex autoimmune disease associated with widespread immune dysregulation and diverse clinical features. Immune abnormalities might be differentially associated with specific organ involvement or response to targeted therapies. We aimed to identify biomarkers of response to belimumab after rituximab to facilitate a personalised approach to therapy.
Methods: In this exploratory analysis of a randomised controlled trial (BEAT-LUPUS), we investigated immune profiles of patients with SLE recruited to the 52-week clinical trial, which tested the combination of rituximab plus belimumab versus rituximab plus placebo. We used machine learning and conventional statistics to investigate relevant laboratory and clinical biomarkers associated with major clinical response. BEAT LUPUS is registered at ISRCTN, 47873003, and is now complete.
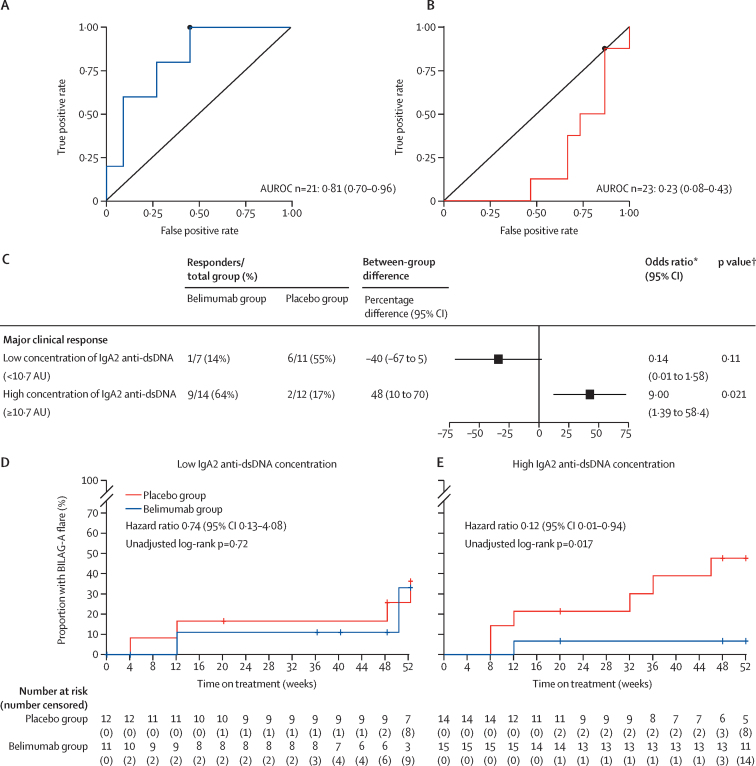
Findings: Between Feb 2, 2017, and March 28, 2019, 52 patients were recruited to BEAT-LUPUS, of whom 44 provided clinical data at week 52 and were included in this analysis. 21 (48%) of 44 participants were in the belimumab group (mean age 39·5 years [SD 12·1]; 17 [81%] were female, four [19%] were male, 13 [62%] were White) and 23 (52%) were in the placebo group (mean age 42·1 years [SD 10·5]; 21 [91%] were female, two [9%] were male, 16 [70%] were White). Ten (48%) of 21 participants who received belimumab after rituximab and eight (35%) of 23 who received placebo after rituximab had a major clinical response at 52 weeks (between-group difference of 13% [95% CI -15 to 38]). We found a predictive association between baseline serum IgA2 anti-double stranded DNA (dsDNA) antibody concentrations and clinical response to belimumab after rituximab, with a between-group difference in major clinical response of 48% (95% CI 10 to 70) in patients with elevated baseline serum IgA2 anti-dsDNA antibody concentrations. Moreover, among those who had a major clinical response, serum IgA2 anti-dsDNA antibody concentrations significantly decreased from baseline only in the belimumab group. Increased circulating IgA2 (but not total) plasmablast numbers, and T follicular helper cell numbers predicted clinical response and were both reduced only in patients who responded to belimumab after rituximab. Serum IgA2 anti-dsDNA antibody concentrations were also associated with active renal disease, whereas serum IgA1 anti-dsDNA antibody and IFN-α concentrations were associated with mucocutaneous disease activity but did not predict response to B-cell targeted therapy. Patients with a high baseline serum interleukin-6 concentration were less likely to have a major clinical response, irrespective of therapy.
Interpretation: This exploratory study revealed the presence of distinct molecular networks associated with renal and mucocutaneous involvement, and response to B-cell-targeted therapies, which, if confirmed, could guide precision targeting of advanced therapies for this heterogenous disease.
Funding: Versus Arthritis, UCLH Biomedical Research Centre, LUPUS UK, and GSK.
© 2023 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license.
Conflict of interest statement
MS and MRE are named on a patent pending (IgA2 anti-dsDNA antibodies as a biomarker in SLE, the patent is to University College London). MRE has received grant support from GSK, VersusArthritis, National Institute of Health and Care Research (NIHR), UK Medical Research Council (MRC), and Lupus UK, on behalf of his coauthors, which funded the research. MRE and CG have been members of the speakers’ bureau for GSK and have received consultancy fees for attending GSK advisory boards. DAI has received consultancy fees from AstraZeneca, Eli Lilly, Merck Serono, Servier. CG also reports personal fees for honoraria from consultancy work from the US Centers for Disease Control and Prevention, AbbVie, Amgen, AstraZeneca, EMD Serono, MGP, Sanofi, and UCB; personal fees for a speakers’ bureau from UCB; and an educational grant from UCB to Sandwell and West Birmingham Hospitals NHS Trust that supported her research work. All other authors declare no competing interests.
Figures




References
-
- Carter LM, Isenberg DA, Ehrenstein MR. Elevated serum BAFF levels are associated with rising anti-double-stranded DNA antibody levels and disease flare following B cell depletion therapy in systemic lupus erythematosus. Arthritis Rheum. 2013;65:2672–2679. - PubMed
-
- Shipa M, Embleton-Thirsk A, Parvaz M, et al. Effectiveness of belimumab after rituximab in systemic lupus erythematosus: a randomized controlled trial. Ann Intern Med. 2021;174:1647–1657. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
