

A critical analysis of neuro-oncology clinical trials
- PMID: 36757281
- PMCID: PMC10484169
- DOI: 10.1093/neuonc/noad036
A critical analysis of neuro-oncology clinical trials
Abstract
Background: Limitations in trial design, accrual, and data reporting impact efficient and reliable drug evaluation in cancer clinical trials. These concerns have been recognized in neuro-oncology but have not been comprehensively evaluated. We conducted a semi-automated survey of adult interventional neuro-oncology trials, examining design, interventions, outcomes, and data availability trends.
Methods: Trials were selected programmatically from ClinicalTrials.gov using primary malignant central nervous system tumor classification terms. Regression analyses assessed design and accrual trends; effect size analysis utilized survival rates among trials investigating survival.
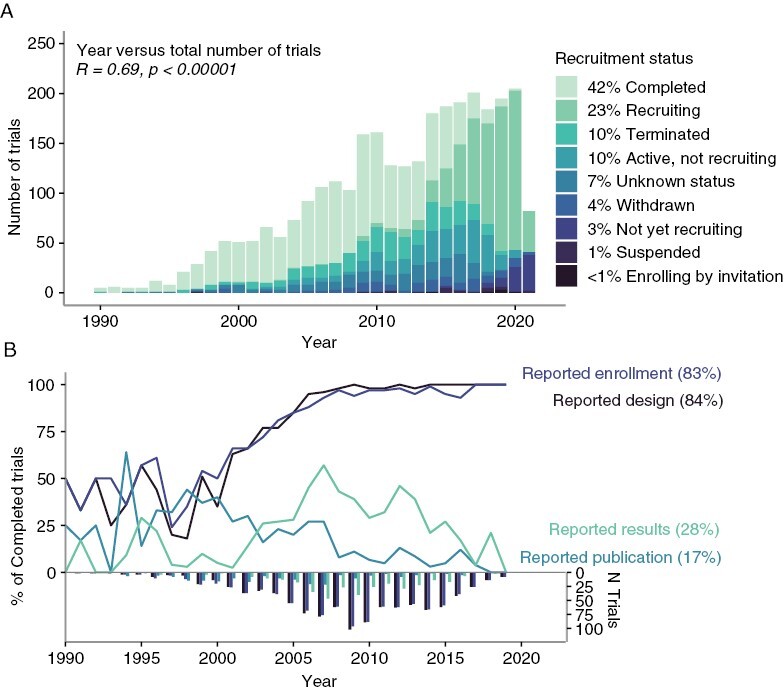
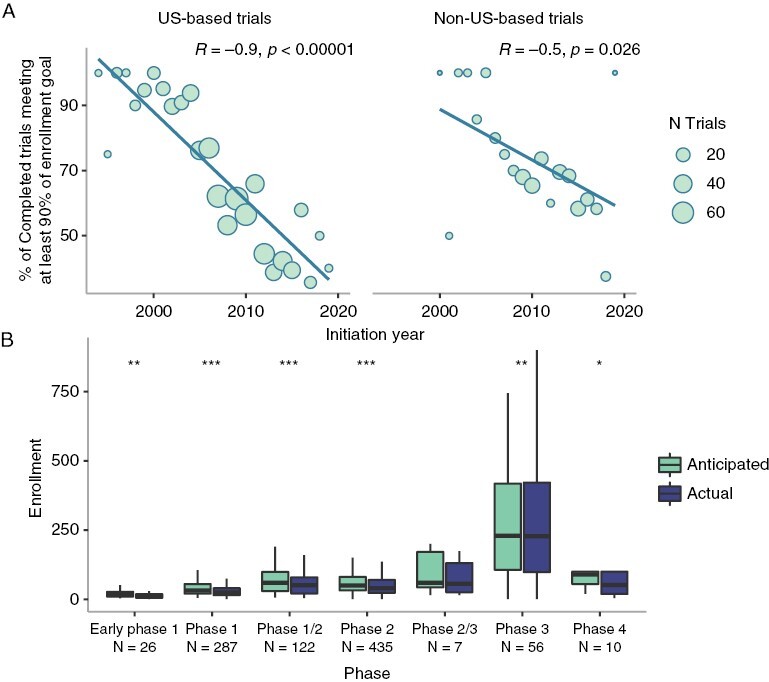
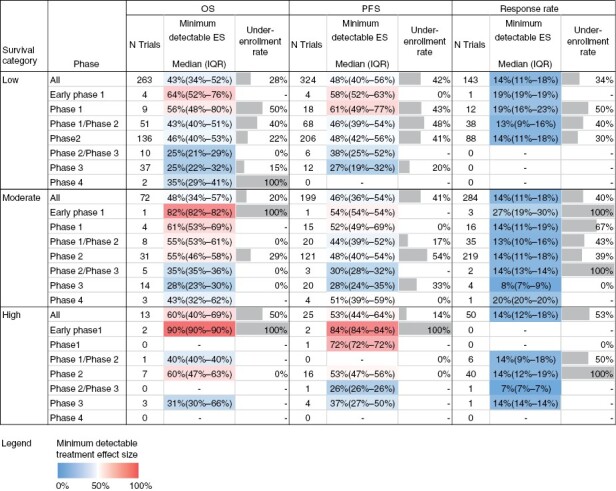
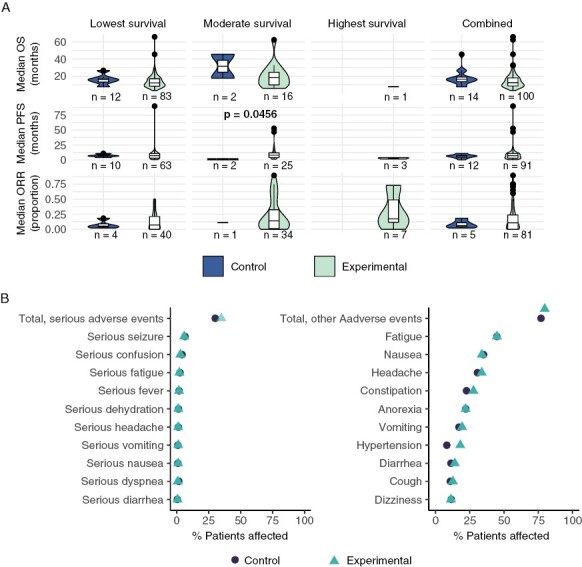
Results: Of 3038 reviewed trials, most trials reporting relevant information were nonblinded (92%), single group (65%), nonrandomized (51%), and studied glioblastomas (47%) or other gliomas. Basic design elements were reported by most trials, with reporting increasing over time (OR = 1.24, P < .00001). Trials assessing survival outcomes were estimated to assume large effect sizes of interventions when powering their designs. Forty-two percent of trials were completed; of these, 38% failed to meet their enrollment target, with worse accrual over time (R = -0.94, P < .00001) and for US versus non-US based trials (OR = 0.5, P < .00001). Twenty-eight percent of completed trials reported partial results, with greater reporting for US (34.6%) versus non-US based trials (9.3%, P < .00001). Efficacy signals were detected by 15%-23% of completed trials reporting survival outcomes.
Conclusion: Low randomization rates, underutilization of controls, and overestimation of effect size, particularly pronounced in early-phase trials, impede generalizability of results. Suboptimal designs may be driven by accrual challenges, underscoring the need for cooperative efforts and novel designs. The limited results reporting highlights the need to incentivize data reporting and harmonization.
Keywords: clinical trial design trends; leveraging of trial registry data; primary central nervous system malignancies; treatment effect size assumptions; trial accrual.
Published by Oxford University Press on behalf of the Society for Neuro-Oncology 2023.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Lapointe S, Perry A, Butowski NA.. Primary brain tumours in adults. Lancet. 2018;392(10145):432–446. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
