

Comparison of the Clinical and Radiological Outcomes of Full-Endoscopic Laminotomy and Conventional Subtotal Laminectomy for Lumbar Spinal Stenosis: A Randomized Controlled Trial
- PMID: 36757395
- PMCID: PMC11268293
- DOI: 10.1177/21925682231155846
Comparison of the Clinical and Radiological Outcomes of Full-Endoscopic Laminotomy and Conventional Subtotal Laminectomy for Lumbar Spinal Stenosis: A Randomized Controlled Trial
Abstract
Study design: Randomized controlled trial.
Objective: The primary objective of this study was to compare the short-term clinical and radiological outcomes of full-endoscopic lumbar laminotomy (FEL) with those of subtotal lumbar laminectomy (STL) for lumbar spinal stenosis (LSS).
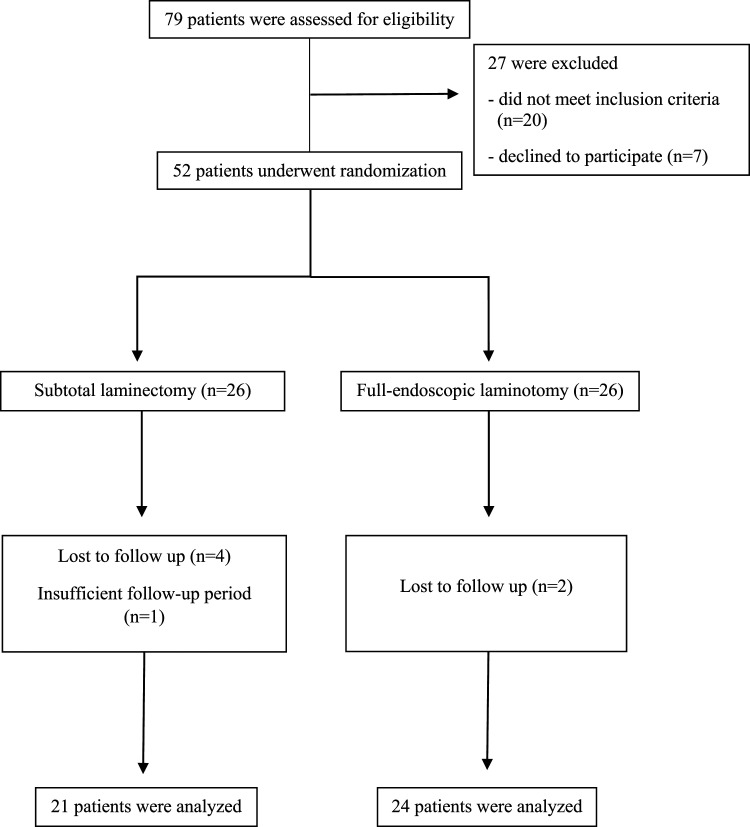
Methods: In this prospective randomized trial a total of 52 patients were enrolled from May 2016 to September 2021 after providing written informed consent. The authors investigated 45 patients who were followed up for more than 6 months.
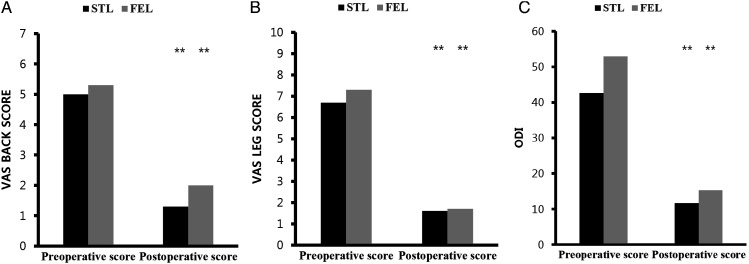
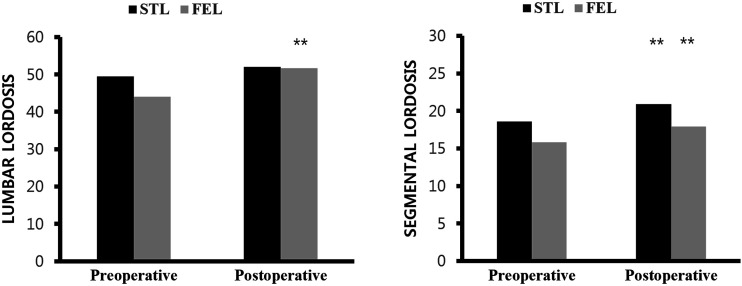
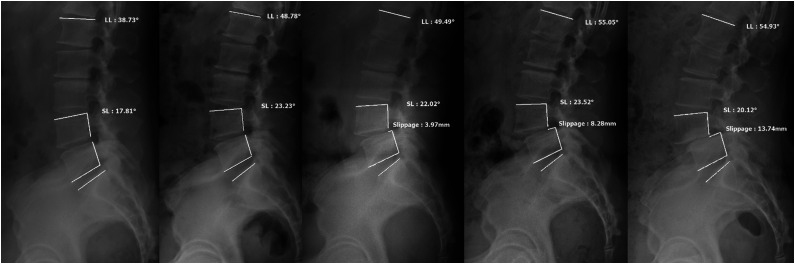
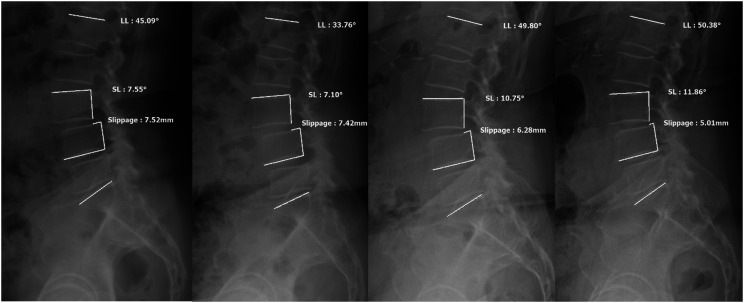
Results: There were significant improvements in visual analogue scale (VAS) and Oswestry Disability Index (ODI) scores after the operation in both groups. The FEL group tended to have significantly shorter hospital stay. Interestingly, a statistically significant increase in postoperative lumbar lordosis and segmental angle was observed in the FEL group and both groups, respectively. Spondylolisthesis was exacerbated or newly developed in five of the 21 patients (24%) in the STL group. In contrast, improvement in spondylolisthesis was observed in two of the 24 patients (8%) in the FEL group. There were no complications that resulted in fatal sequelae and no significant difference in the complication rate.
Conclusions: The clinical results of FEL were similar to those of STL. In addition, the results of FEL were superior to those of STL in terms of a decrease in the postoperative length of stay and radiologic instability, such as iatrogenic spondylolisthesis. The results of this study indicate that FEL is a comparable surgical method to STL for LSS.
Keywords: decompression; endoscopy; full-endoscopy; laminectomy; spinal stenosis; spine; spondylolisthesis.
Conflict of interest statement
Declaration of Conflicting InterestsThe author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The corresponding author, Jin-Sung Kim, is a consultant of RIWOSPINE, Gmbh, Germany, Elliquence, LLC, USA. The other authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures

References
-
- Deyo RA, Mirza SK, Martin BI. Back pain prevalence and visit rates: estimates from U.S. national surveys. Spine (Phila Pa 1976). 2002;31(23):2724-2727. doi:10.1097/01.brs.0000244618.06877.cd. - DOI - PubMed
LinkOut - more resources
Full Text Sources
