

Stabilization of E-cadherin adhesions by COX-2/GSK3β signaling is a targetable pathway in metastatic breast cancer
- PMID: 36757813
- PMCID: PMC10070121
- DOI: 10.1172/jci.insight.156057
Stabilization of E-cadherin adhesions by COX-2/GSK3β signaling is a targetable pathway in metastatic breast cancer
Abstract
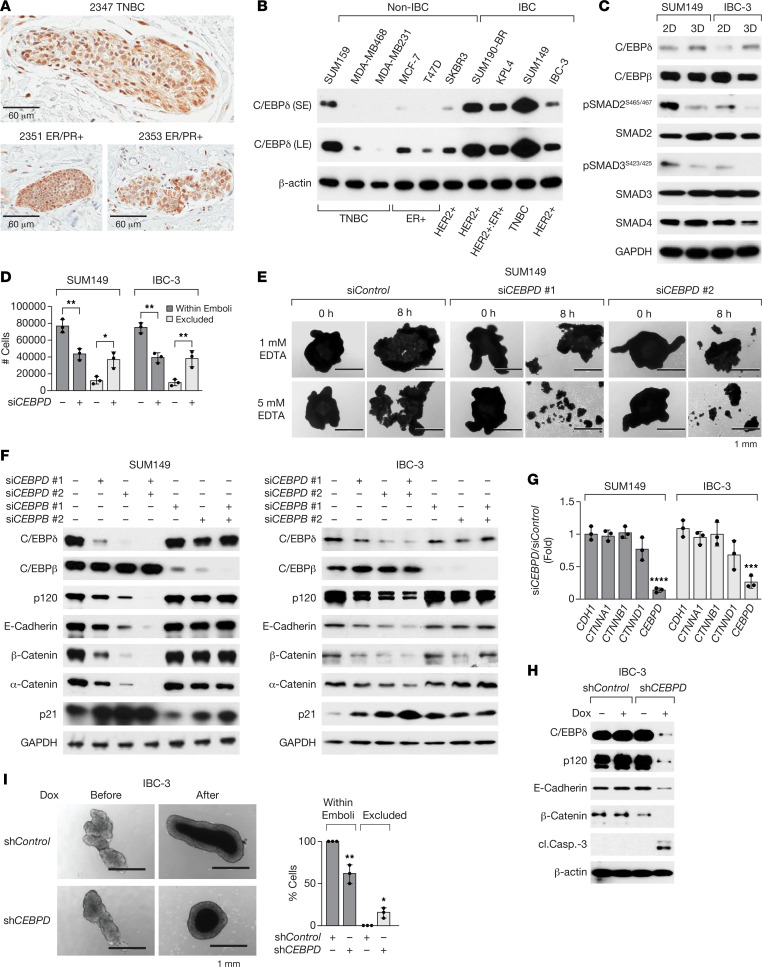
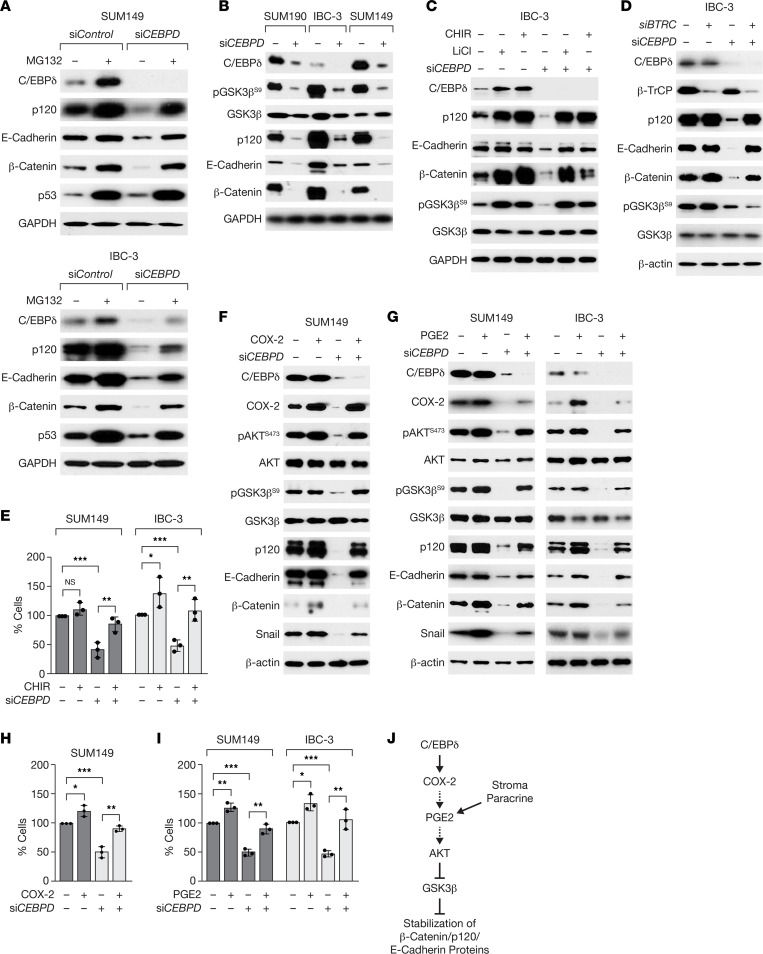
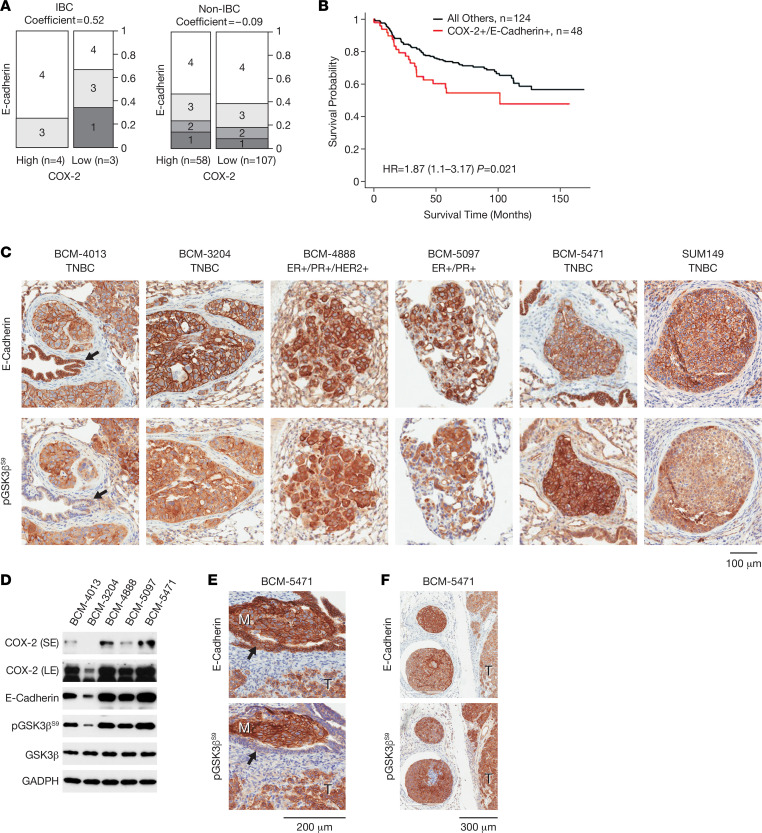
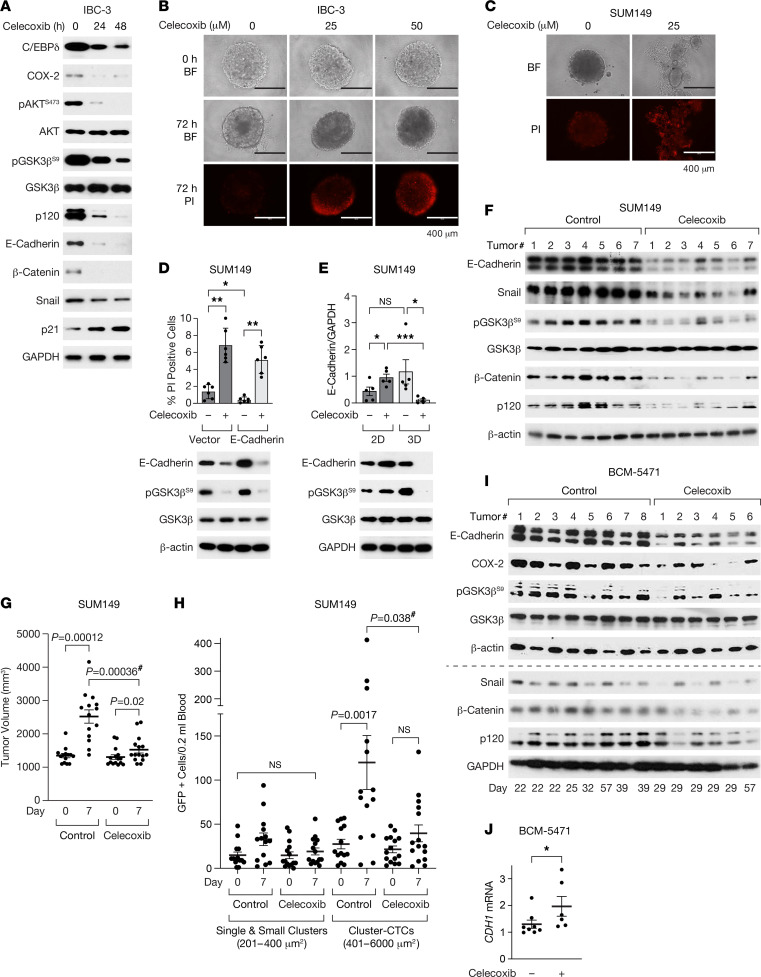
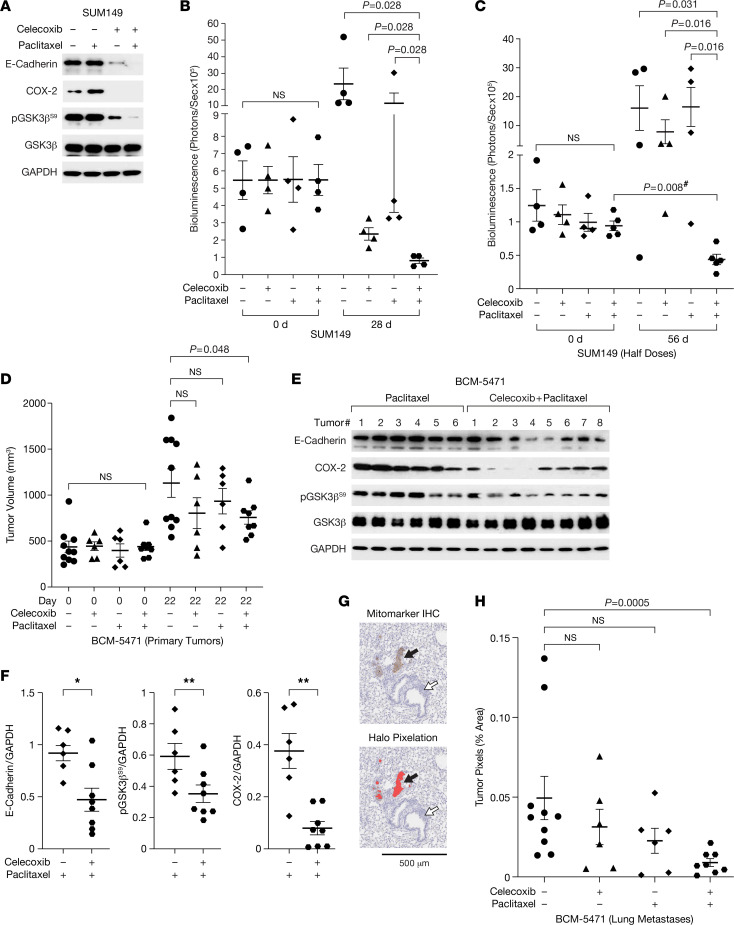
Metastatic progression of epithelial cancers can be associated with epithelial-mesenchymal transition (EMT) including transcriptional inhibition of E-cadherin (CDH1) expression. Recently, EM plasticity (EMP) and E-cadherin-mediated, cluster-based metastasis and treatment resistance have become more appreciated. However, the mechanisms that maintain E-cadherin expression in this context are less understood. Through studies of inflammatory breast cancer (IBC) and a 3D tumor cell "emboli" culture paradigm, we discovered that cyclooxygenase 2 (COX-2; PTGS2), a target gene of C/EBPδ (CEBPD), or its metabolite prostaglandin E2 (PGE2) promotes protein stability of E-cadherin, β-catenin, and p120 catenin through inhibition of GSK3β. The COX-2 inhibitor celecoxib downregulated E-cadherin complex proteins and caused cell death. Coexpression of E-cadherin and COX-2 was seen in breast cancer tissues from patients with poor outcome and, along with inhibitory GSK3β phosphorylation, in patient-derived xenografts (PDX) including triple negative breast cancer (TNBC).Celecoxib alone decreased E-cadherin protein expression within xenograft tumors, though CDH1 mRNA levels increased, and reduced circulating tumor cell (CTC) clusters. In combination with paclitaxel, celecoxib attenuated or regressed lung metastases. This study has uncovered a mechanism by which metastatic breast cancer cells can maintain E-cadherin-mediated cell-to-cell adhesions and cell survival, suggesting that some patients with COX-2+/E-cadherin+ breast cancer may benefit from targeting of the PGE2 signaling pathway.
Keywords: Breast cancer; Cell Biology; Cell migration/adhesion; Oncology; Signal transduction.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
