

A streamlined, machine learning-derived approach to risk-stratification in heart failure patients with secondary tricuspid regurgitation
- PMID: 36757905
- PMCID: PMC10125224
- DOI: 10.1093/ehjci/jead009
A streamlined, machine learning-derived approach to risk-stratification in heart failure patients with secondary tricuspid regurgitation
Abstract
Aims: Secondary tricuspid regurgitation (sTR) is the most frequent valvular heart disease and has a significant impact on mortality. A high burden of comorbidities often worsens the already dismal prognosis of sTR, while tricuspid interventions remain underused and initiated too late. The aim was to examine the most powerful predictors of all-cause mortality in moderate and severe sTR using machine learning techniques and to provide a streamlined approach to risk-stratification using readily available clinical, echocardiographic and laboratory parameters.
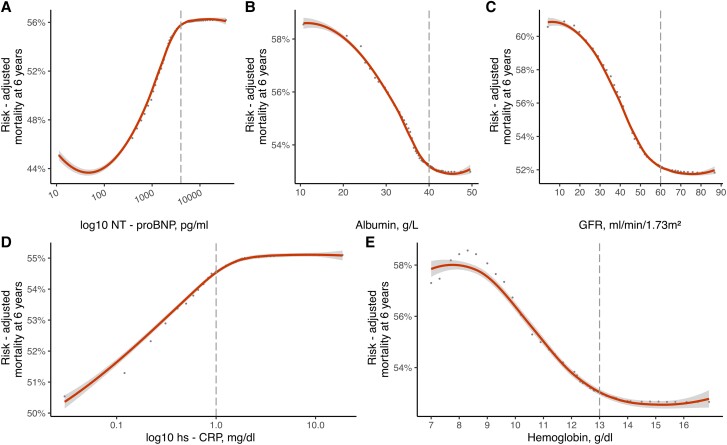
Methods and results: This large-scale, long-term observational study included 3359 moderate and 1509 severe sTR patients encompassing the entire heart failure spectrum (preserved, mid-range and reduced ejection fraction). A random survival forest was applied to investigate the most important predictors and group patients according to their number of adverse features.The identified predictors and thresholds, that were associated with significantly worse mortality were lower glomerular filtration rate (<60 mL/min/1.73m2), higher NT-proBNP, increased high sensitivity C-reactive protein, serum albumin < 40 g/L and hemoglobin < 13 g/dL. Additionally, grouping patients according to the number of adverse features yielded important prognostic information, as patients with 4 or 5 adverse features had a fourfold risk increase in moderate sTR [4.81(3.56-6.50) HR 95%CI, P < 0.001] and fivefold risk increase in severe sTR [5.33 (3.28-8.66) HR 95%CI, P < 0.001].
Conclusion: This study presents a streamlined, machine learning-derived and internally validated approach to risk-stratification in patients with moderate and severe sTR, that adds important prognostic information to aid clinical-decision-making.
Keywords: HFmrEF; HFpEF; HFrEF; machine learning; secondary tricuspid regurgitation.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: None declared.
Figures




References
-
- Topilsky Y, Maltais S, Medina Inojosa J, Oguz D, Michelena H, Maalouf Jet al. . Burden of tricuspid regurgitation in patients diagnosed in the community setting. JACC Cardiovasc Imaging 2019;12:433–42. - PubMed
-
- Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachs Jet al. . ESC/EACTS guidelines for the management of valvular heart disease: developed by the Task Force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 2021;2021.
-
- Antunes MJ, Rodriguez-Palomares J, Prendergast B, De Bonis M, Rosenhek R, Al-Attar Net al. . Management of tricuspid valve regurgitation: position statement of the European Society of Cardiology Working Groups of Cardiovascular Surgery and Valvular Heart Disease. Eur J Cardiothorac Surg 2017;52:1022–30. - PubMed
-
- Bartko PE, Arfsten H, Frey MK, Heitzinger G, Pavo N, Cho Aet al. . Natural history of functional tricuspid regurgitation: implications of quantitative Doppler assessment. JACC Cardiovasc Imaging 2019;12:389–97. - PubMed
-
- Spinka G, Bartko PE, Heitzinger G, Prausmuller S, Pavo N, Frey MKet al. . Natural course of nonsevere secondary tricuspid regurgitation. J Am Soc Echocardiogr 2021;34:13–19. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
