

Segmental motor recovery after cervical spinal cord injury relates to density and integrity of corticospinal tract projections
- PMID: 36759606
- PMCID: PMC9911610
- DOI: 10.1038/s41467-023-36390-7
Segmental motor recovery after cervical spinal cord injury relates to density and integrity of corticospinal tract projections
Abstract
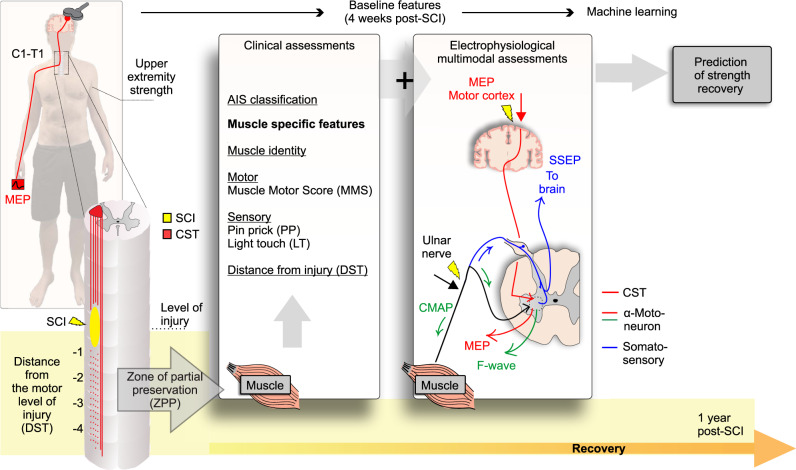
Cervical spinal cord injury (SCI) causes extensive impairments for individuals which may include dextrous hand function. Although prior work has focused on the recovery at the person-level, the factors determining the recovery of individual muscles are poorly understood. Here, we investigate the muscle-specific recovery after cervical spinal cord injury in a retrospective analysis of 748 individuals from the European Multicenter Study about Spinal Cord Injury (NCT01571531). We show associations between corticospinal tract (CST) sparing and upper extremity recovery in SCI, which improves the prediction of hand muscle strength recovery. Our findings suggest that assessment strategies for muscle-specific motor recovery in acute spinal cord injury are improved by accounting for CST sparing, and complement person-level predictions.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures







References
-
- Ahuja CS, et al. Traumatic spinal cord injury. Nat. Rev. Dis. Prim. 2017;3:17018. - PubMed
-
- Snoek GJ, Ijzerman MJ, Hermens HJ, Maxwell D, Biering-Sorensen F. Survey of the needs of patients with spinal cord injury: Impact and priority for improvement in hand function in tetraplegics. Spinal Cord. 2004;42:526–532. - PubMed
-
- Fawcett JW, et al. Guidelines for the conduct of clinical trials for spinal cord injury as developed by the ICCP panel: Spontaneous recovery after spinal cord injury and statistical power needed for therapeutic clinical trials. Spinal Cord. 2007;45:190–205. - PubMed
-
- Hupp M, Pavese C, Bachmann LM, Koller R, Schubert M. Electrophysiological Multimodal Assessments Improve Outcome Prediction in Traumatic Cervical Spinal Cord Injury. J. Neurotrauma. 2018;35:2916–2923. - PubMed
-
- Khorasanizadeh MH, et al. Neurological recovery following traumatic spinal cord injury: A systematic review and meta-analysis. J. Neurosurg. Spine. 2019;30:683–699. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
