

Elevated plasma interleukin-8 as a risk factor for mortality in children presenting with cerebral malaria
- PMID: 36759905
- PMCID: PMC9909955
- DOI: 10.1186/s40249-023-01059-2
Elevated plasma interleukin-8 as a risk factor for mortality in children presenting with cerebral malaria
Abstract
Background: Cerebral malaria (CM) is a neuropathology which remains one of the deadliest forms of malaria among African children. The kinetics of the pathophysiological mechanisms leading to neuroinflammation and the death or survival of patients during CM are still poorly understood. The increasing production of cytokines, chemokines and other actors of the inflammatory and oxidative response by various local actors in response to neuroinflammation plays a major role during CM, participating in both the amplification of the neuroinflammation phenomenon and its resolution. In this study, we aimed to identify risk factors for CM death among specific variables of inflammatory and oxidative responses to improve our understanding of CM pathogenesis.
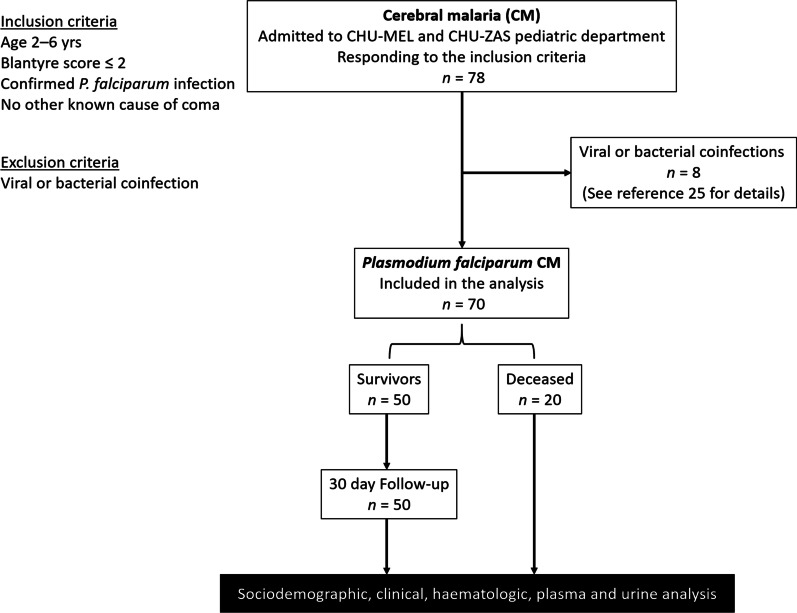
Methods: Children presenting with CM (n = 70) due to P. falciparum infection were included in southern Benin and divided according to the clinical outcome into 50 children who survived and 20 who died. Clinical examination was complemented by fundoscopic examination and extensive blood biochemical analysis associated with molecular diagnosis by multiplex PCR targeting 14 pathogens in the patients' cerebrospinal fluid to rule out coinfections. Luminex technology and enzyme immunoassay kits were used to measure 17 plasma and 7 urinary biomarker levels, respectively. Data were analysed by univariate analysis using the nonparametric Mann‒Whitney U test and Pearson's Chi2 test. Adjusted and multivariate analyses were conducted separately for plasma and urinary biomarkers to identify CM mortality risk factors.
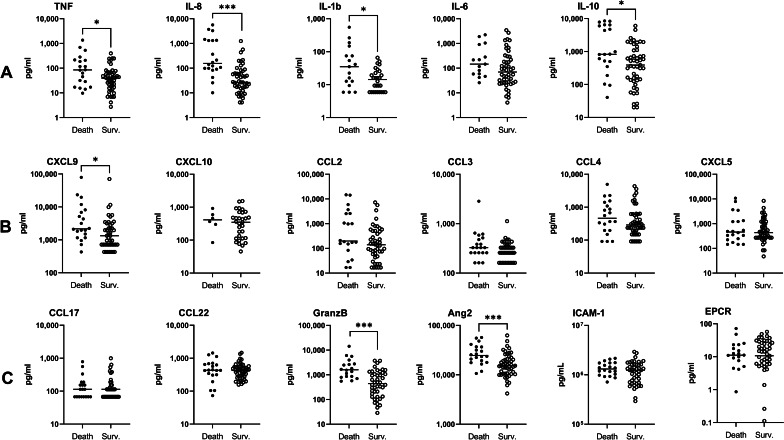
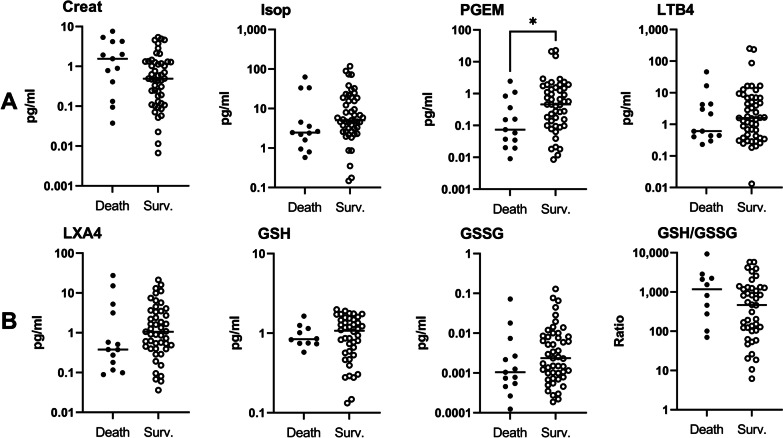
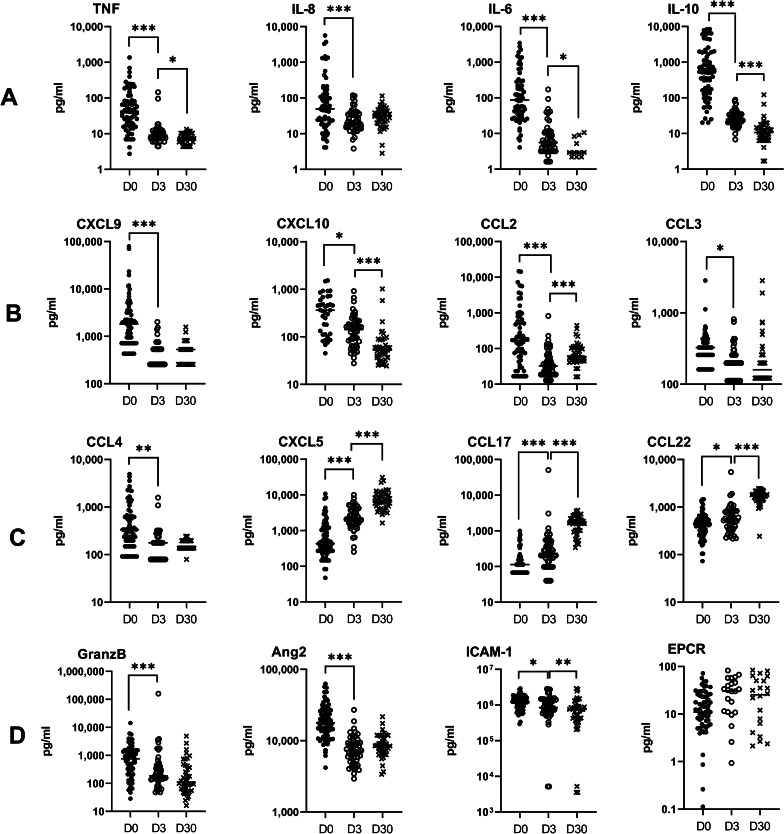
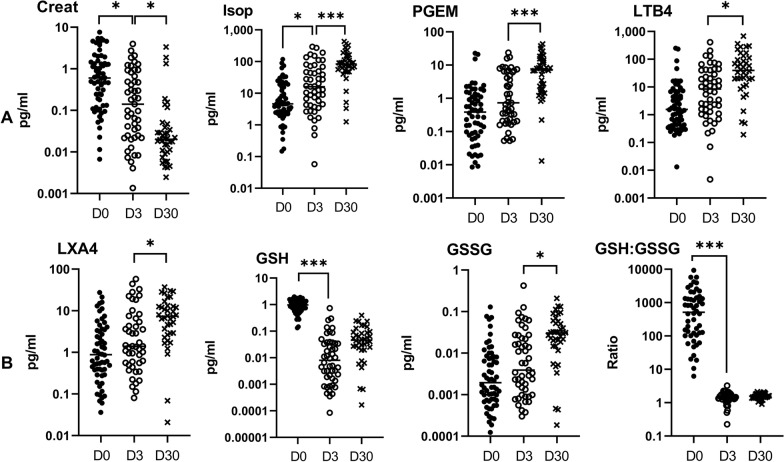
Results: Univariate analysis revealed higher plasma levels of tumour necrosis factor (TNF), interleukin-1beta (IL-1β), IL-10, IL-8, C-X-C motif chemokine ligand 9 (CXCL9), granzyme B, and angiopoietin-2 and lower urinary levels of prostanglandine E2 metabolite (PGEM) in children who died compared to those who survived CM (Mann-Whitney U-test, P-values between 0.03 and < 0.0001). The multivariate logistic analysis highlighted elevated plasma levels of IL-8 as the main risk factor for death during CM (adjusted odd ratio = 14.2, P-value = 0.002). Values obtained during follow-up at D3 and D30 revealed immune factors associated with disease resolution, including plasma CXCL5, C-C motif chemokine ligand 17 (CCL17), CCL22, and urinary 15-F2t-isoprostane.
Conclusions: The main risk factor of death during CM was thus elevated plasma levels of IL-8 at inclusion. Follow-up of patients until D30 revealed marker profiles of disease aggravation and resolution for markers implicated in neutrophil activation, endothelium activation and damage, inflammatory and oxidative response. These results provide important insight into our understanding of CM pathogenesis and clinical outcome and may have important therapeutic implications.
Keywords: Benin; Cerebral malaria; Children; Cytokine; Immunologic marker; NeuroCM; Plasma; Urine.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- World health Organization . World malaria report. Geneva: World health Organization; 2020.
-
- World health Organization . Management of severe malaria: a practical handbook. 3. Geneva: World health Organization; 2012.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
