

Changes in epicardial and visceral adipose tissue depots following bariatric surgery and their effect on cardiac geometry
- PMID: 36761185
- PMCID: PMC9905224
- DOI: 10.3389/fendo.2023.1092777
Changes in epicardial and visceral adipose tissue depots following bariatric surgery and their effect on cardiac geometry
Abstract
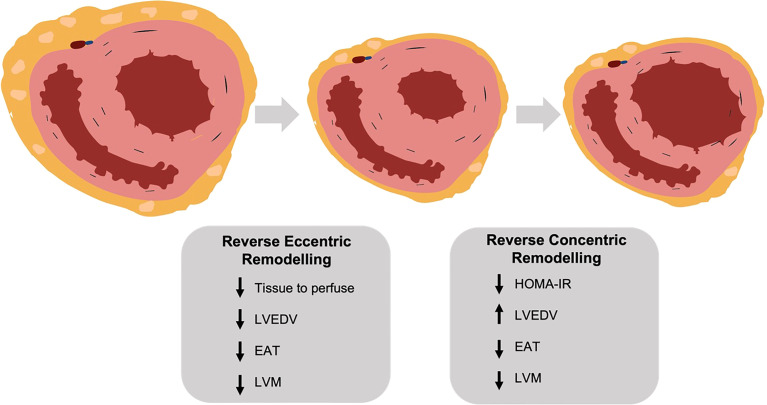
Introduction: Obesity affects cardiac geometry, causing both eccentric (due to increased cardiac output) and concentric (due to insulin resistance) remodelling. Following bariatric surgery, reversal of both processes should occur. Furthermore, epicardial adipose tissue loss following bariatric surgery may reduce pericardial restraint, allowing further chamber expansion. We investigated these changes in a serial imaging study of adipose depots and cardiac geometry following bariatric surgery.
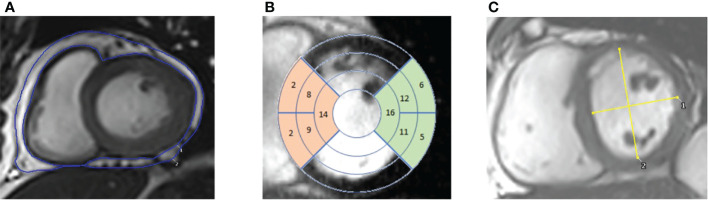
Methods: 62 patients underwent cardiac magnetic resonance (CMR) before and after bariatric surgery, including 36 with short-term (median 212 days), 37 medium-term (median 428 days) and 32 long-term (median 1030 days) follow-up. CMR was used to assess cardiac geometry (left atrial volume (LAV) and left ventricular end-diastolic volume (LVEDV)), LV mass (LVM) and LV eccentricity index (LVei - a marker of pericardial restraint). Abdominal visceral (VAT) and epicardial (EAT) adipose tissue were also measured.
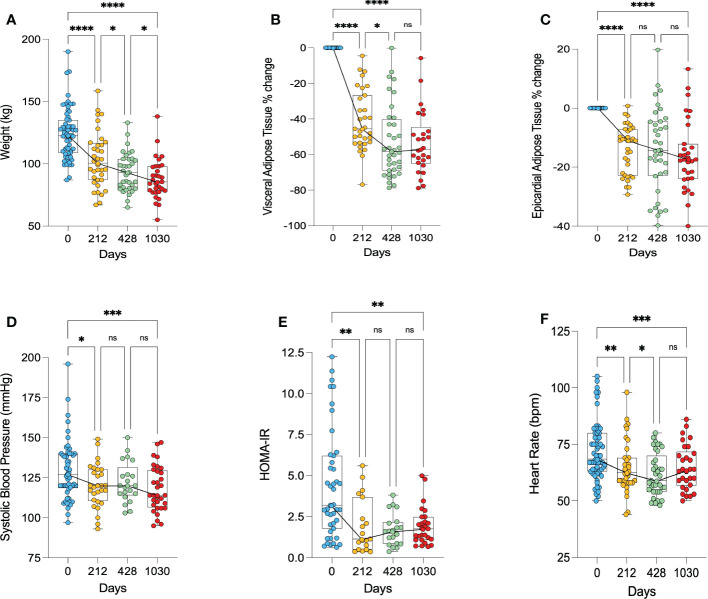
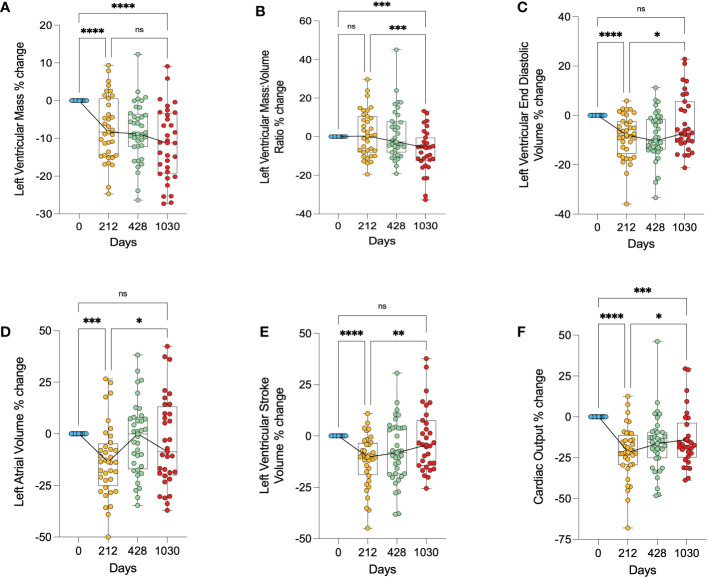
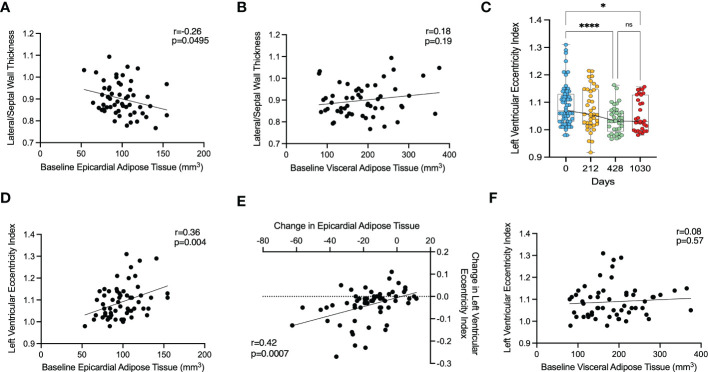
Results: Patients on average had lost 21kg (38.9% excess weight loss, EWL) at 212 days and 36kg (64.7% EWL) at 1030 days following bariatric surgery. Most VAT and EAT loss (43% and 14%, p<0.0001) occurred within the first 212 days, with non-significant reductions thereafter. In the short-term LVM (7.4%), LVEDV (8.6%) and LAV (13%) all decreased (all p<0.0001), with change in cardiac output correlated with LVEDV (r=0.35,p=0.03) and LAV change (r=0.37,p=0.03). Whereas LVM continued to decrease with time (12% decrease relative to baseline at 1030 days, p<0.0001), both LAV and LVEDV had returned to baseline by 1030 days. LV mass:volume ratio (a marker of concentric hypertrophy) reached its nadir at the longest timepoint (p<0.001). At baseline, LVei correlated with baseline EAT (r=0.37,p=0.0040), and decreased significantly from 1.09 at baseline to a low of 1.04 at 428 days (p<0.0001). Furthermore, change in EAT following bariatric surgery correlated with change in LVei (r=0.43,p=0.0007).
Conclusions: Cardiac volumes show a biphasic response to weight loss, initially becoming smaller and then returning to pre-operative sizes by 1030 days. We propose this is due to an initial reversal of eccentric remodelling followed by reversal of concentric remodelling. Furthermore, we provide evidence for a role of EAT contributing to pericardial restraint, with EAT loss improving markers of pericardial restraint.
Trial registration: ClinicalTrials.gov NCT01284816.
Keywords: bariatric surgery; cardiac geometry; cardiac remodelling; epicardiac adipose tissue; obesity; weight loss.
Copyright © 2023 Henry, Abdesselam, Deal, Lewis, Rayner, Bernard, Dutour, Gaborit, Kober, Soghomonian, Sgromo, Byrne, Bege, Neubauer, Borlaug and Rider.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
The effect of bariatric surgery type on cardiac reverse remodelling.Int J Obes (Lond). 2024 Jun;48(6):808-814. doi: 10.1038/s41366-024-01474-x. Epub 2024 Jan 31. Int J Obes (Lond). 2024. PMID: 38297029 Free PMC article.
-
Open-bore MRI Scanner Assessment of Epicardial Adipose Tissue after Bariatric Surgery: A Pilot Study.Endocr Metab Immune Disord Drug Targets. 2025;25(2):173-188. doi: 10.2174/0118715303310680240607114244. Endocr Metab Immune Disord Drug Targets. 2025. PMID: 39171595 Free PMC article.
-
Long-Term Changes in Cardiac Structure and Function Following Bariatric Surgery.J Am Coll Cardiol. 2022 Oct 18;80(16):1501-1512. doi: 10.1016/j.jacc.2022.08.738. J Am Coll Cardiol. 2022. PMID: 36229085 Free PMC article.
-
Targeting epicardial adipose tissue with exercise, diet, bariatric surgery or pharmaceutical interventions: A systematic review and meta-analysis.Obes Rev. 2021 Jan;22(1):e13136. doi: 10.1111/obr.13136. Epub 2020 Sep 8. Obes Rev. 2021. PMID: 32896056
-
Visceral adiposity and inflammatory bowel disease.Int J Colorectal Dis. 2021 Nov;36(11):2305-2319. doi: 10.1007/s00384-021-03968-w. Epub 2021 Jun 9. Int J Colorectal Dis. 2021. PMID: 34104989 Review.
Cited by
-
Abdominal obesity is associated with increased worsening renal function risk in patients with heart failure with preserved ejection fraction.BMC Cardiovasc Disord. 2024 Sep 9;24(1):477. doi: 10.1186/s12872-024-04118-0. BMC Cardiovasc Disord. 2024. PMID: 39251903 Free PMC article. Clinical Trial.
-
Fluctuations of epicardial adipose tissue and cardiovascular health: A useful biomarker? A comprehensive review.J Cardiovasc Thorac Res. 2025 Jun 28;17(2):80-90. doi: 10.34172/jcvtr.025.33332. eCollection 2025 Jun. J Cardiovasc Thorac Res. 2025. PMID: 40862097 Free PMC article. Review.
-
Epicardial adipose tissue, metabolic disorders, and cardiovascular diseases: recent advances classified by research methodologies.MedComm (2020). 2023 Oct 24;4(6):e413. doi: 10.1002/mco2.413. eCollection 2023 Dec. MedComm (2020). 2023. PMID: 37881786 Free PMC article. Review.
-
The role of epicardial adipose tissue remodelling in heart failure with preserved ejection fraction.Cardiovasc Res. 2025 Jun 12;121(6):860-870. doi: 10.1093/cvr/cvaf056. Cardiovasc Res. 2025. PMID: 40238568 Free PMC article. Review.
-
Reductions in Epicardial Adipose Tissue and Mediastinal Fat Are Associated with Improved Cardiac Function.Obes Surg. 2025 Aug;35(8):2854-2866. doi: 10.1007/s11695-025-08000-6. Epub 2025 Jul 5. Obes Surg. 2025. PMID: 40616623 Free PMC article.
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical