

The efficacy and safety of quinagolide in hyperprolactinemia treatment: A systematic review and meta-analysis
- PMID: 36761195
- PMCID: PMC9902948
- DOI: 10.3389/fendo.2023.1027905
The efficacy and safety of quinagolide in hyperprolactinemia treatment: A systematic review and meta-analysis
Abstract
Purpose: Three dopamine agonists [bromocriptine, cabergoline, and quinagolide (CV)] have been used for hyperprolactinemia treatment for decades. Several studies have reviewed the efficacy and safety of bromocriptine and cabergoline. However, no systematic review or meta-analysis has discussed the efficacy and safety of CV in hyperprolactinemia and prolactinoma treatment.
Methods: Five medical databases (PubMed, Web of Science, Embase, Scopus, and Cochrane Library) were searched up to 9 May 2022 to identify studies related to CV and hyperprolactinemia. A meta-analysis was implemented by using a forest plot, funnel plot, sensitivity analysis, meta-regression, and Egger's test via software R 4.0 and STATA 12.
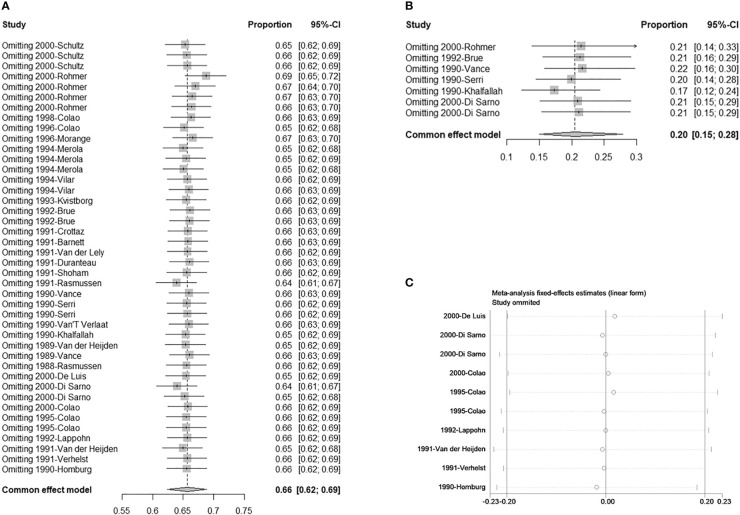
Results: A total of 1,211 studies were retrieved from the five medical databases, and 33 studies consisting of 827 patients were finally included in the analysis. The pooled proportions of patients with prolactin concentration normalization and tumor reduction (>50%) under CV treatment were 69% and 20%, respectively, with 95% confidence intervals of 61%-76% and 15%-28%, respectively. The pooled proportion of adverse effects was 13%, with a 95% confidence interval of 11%-16%.
Conclusion: Our study showed that CV is not less effective than cabergoline and bromocriptine in treating hyperprolactinemia, and the side effects were not significant. Hence, this drug could be considered an alternative first-line or rescue treatment in treating hyperprolactinemia in the future.
Systematic review registration: https://www.crd.york.ac.uk/PROSPERO, identifier CRD42022347750.
Keywords: bromocriptine; cabergoline; dopamine agonist; efficacy; hyperprolactinemia; meta-analysis; prolactinomas; quinagolide.
Copyright © 2023 Zeng, Huang, Zou, Tan, Zhou and Li.
Conflict of interest statement
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Figures




Similar articles
-
The recurrence of prolactinoma after withdrawal of dopamine agonist: a systematic review and meta-analysis.BMC Endocr Disord. 2021 Nov 13;21(1):225. doi: 10.1186/s12902-021-00889-1. BMC Endocr Disord. 2021. PMID: 34774043 Free PMC article.
-
A comparative review of the tolerability profiles of dopamine agonists in the treatment of hyperprolactinaemia and inhibition of lactation.Drug Saf. 1996 Apr;14(4):228-38. doi: 10.2165/00002018-199614040-00003. Drug Saf. 1996. PMID: 8713691 Review.
-
The effect of quinagolide and cabergoline, two selective dopamine receptor type 2 agonists, in the treatment of prolactinomas.Clin Endocrinol (Oxf). 2000 Jul;53(1):53-60. doi: 10.1046/j.1365-2265.2000.01016.x. Clin Endocrinol (Oxf). 2000. PMID: 10931080 Clinical Trial.
-
Hyperprolactinemia: pathophysiology and management.Treat Endocrinol. 2003;2(1):23-32. doi: 10.2165/00024677-200302010-00003. Treat Endocrinol. 2003. PMID: 15871552 Review.
-
Prolactinomas resistant to bromocriptine: long-term efficacy of quinagolide and outcome of pregnancy.Eur J Endocrinol. 1996 Oct;135(4):413-20. doi: 10.1530/eje.0.1350413. Eur J Endocrinol. 1996. PMID: 8921822
Cited by
-
Sini San ameliorates lipid metabolism in hyperprolactinemia rat with liver-depression.Curr Res Food Sci. 2024 Sep 14;9:100853. doi: 10.1016/j.crfs.2024.100853. eCollection 2024. Curr Res Food Sci. 2024. PMID: 39328388 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical