

Rescue intracranial stenting for acute ischemic stroke after the failure of mechanical thrombectomy: A systematic review, meta-analysis, and trial sequential analysis
- PMID: 36761342
- PMCID: PMC9905111
- DOI: 10.3389/fneur.2023.1023089
Rescue intracranial stenting for acute ischemic stroke after the failure of mechanical thrombectomy: A systematic review, meta-analysis, and trial sequential analysis
Abstract
Background: Intracranial rescue stenting (RS) might be an option for acute ischemic stroke after the failure of mechanical thrombectomy (MT). However, the findings were not consistent in previous systematic reviews, and whether the conclusion was supported by sufficient statistical power is unknown.
Aim: To examine the effect of RS on acute ischemic stroke after the failure of MT with a systematic review, meta-analysis, and trial sequential analysis (TSA).
Methods: We searched Ovid Medline, Embase, and the Cochrane Central Register of Controlled Trials (CENTRAL) from inception to 15 June 2022, without any language restriction. Studies assessing the effect of RS for acute ischemia stroke after MT failure were included. Two reviewers independently screened the retrieved articles, extracted data, and evaluated the quality of the included studies through the New Ottawa Scale (NOS). The primary outcome was the recanalization rate after RS. Secondary outcomes included modified Rankin Scale (mRS) at 3 months after stroke, symptomatic intracranial hemorrhage (sICH), and mortality rate. We synthesized the data through a random-effects model and performed a TSA analysis.
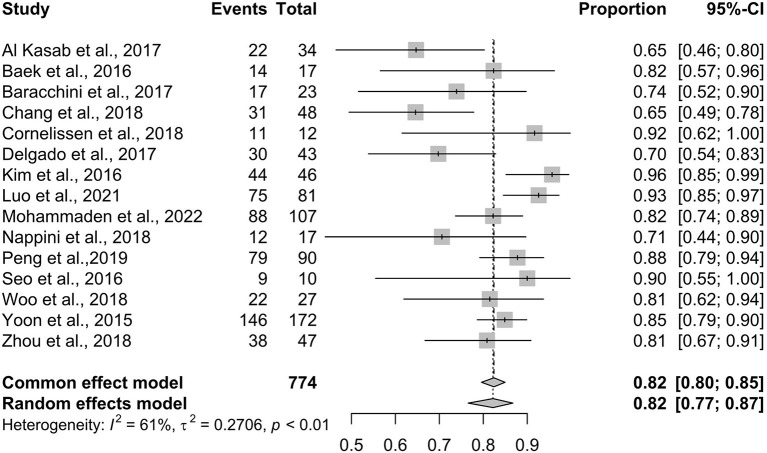
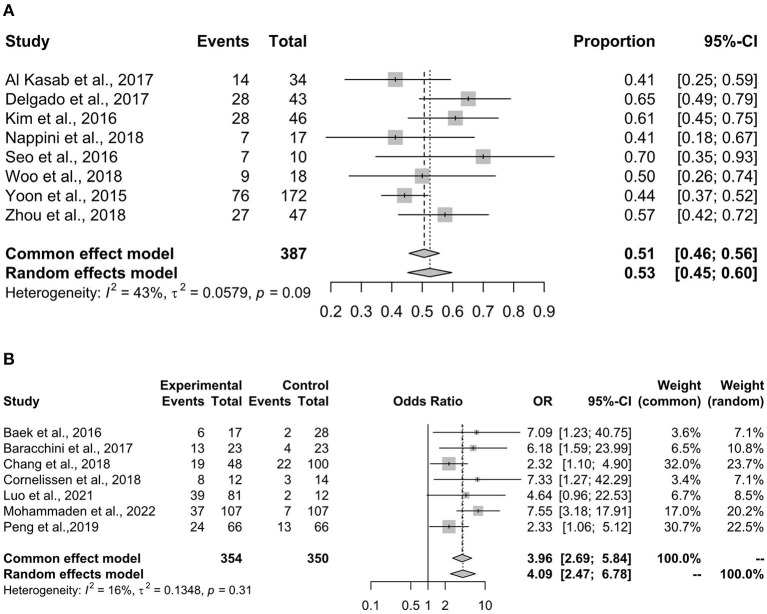
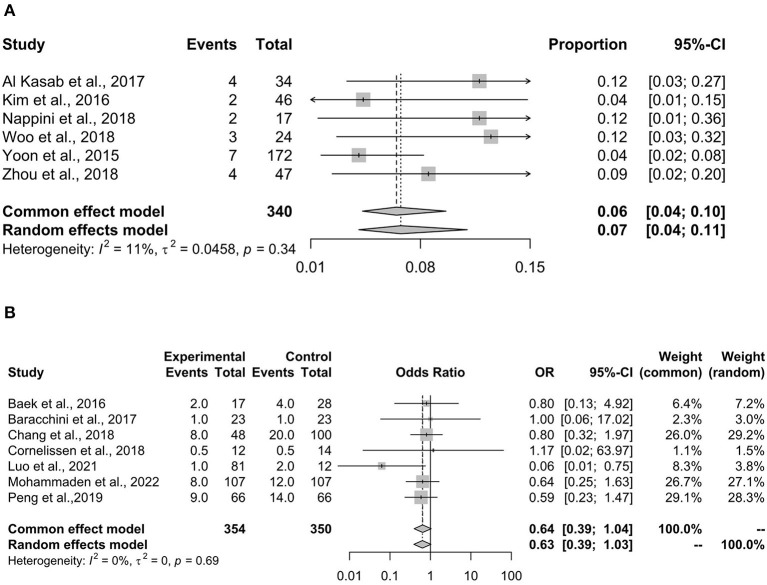
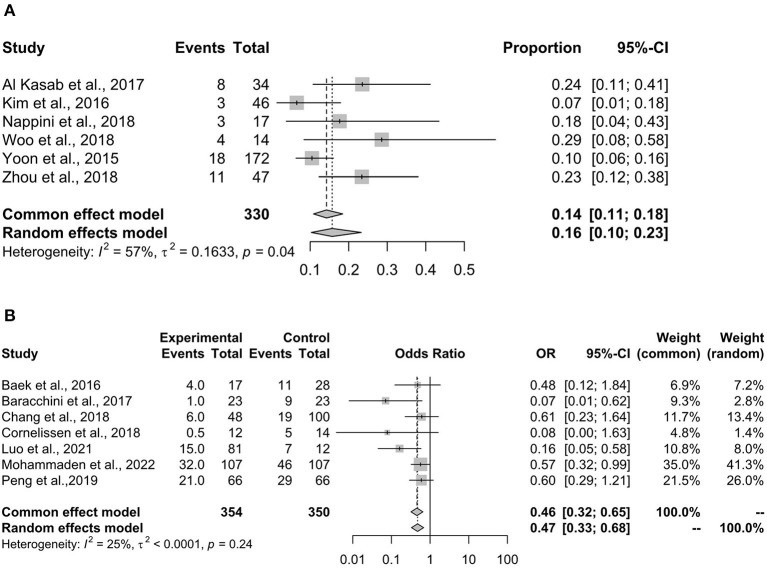
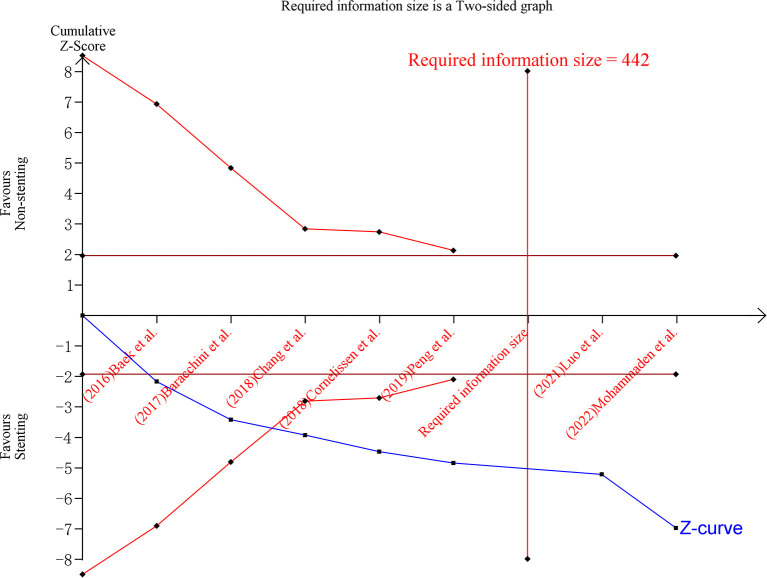
Results: We included 15 studies (containing 1,595 participants) after screening 3,934 records. The pooled recanalization rate for rescue stenting was 82% (95% CI 77-87%). Compared with non-stenting, rescue stenting was associated with a higher proportion of patients with 0-2 mRS score (OR 3.96, 95% CI 2.69-5.84, p < 0.001) and a lower 90-day mortality rate (OR 0.46, 95% CI 0.32-0.65, p < 0.001), and stenting did not increase sICH rate (OR 0.63, 95% CI 0.39-1.04, p = 0.075). The TSA analysis showed that the meta-analysis of the mRS score had a sufficient sample size and statistical power.
Conclusions: Our study showed that rescue stenting was effective and safe for patients with acute ischemia stroke who also had a failed MT, and this result was confirmed in a TSA analysis.
Keywords: acute ischemic stroke; mechanical thrombectomy failure; meta-analysis; rescue stenting; trial sequential analysis.
Copyright © 2023 Cai, Xu, Xiao, Hu, Xu, Guo, Xie, Pan, Tang, Gong, Liu, Su, Deng and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Rescue Intracranial Stenting After Failed Mechanical Thrombectomy for Acute Ischemic Stroke: A Systematic Review and Meta-Analysis.World Neurosurg. 2019 Dec;132:e235-e245. doi: 10.1016/j.wneu.2019.08.192. Epub 2019 Sep 5. World Neurosurg. 2019. PMID: 31493593
-
Stenting and Angioplasty in Neurothrombectomy: Matched Analysis of Rescue Intracranial Stenting Versus Failed Thrombectomy.Stroke. 2022 Sep;53(9):2779-2788. doi: 10.1161/STROKEAHA.121.038248. Epub 2022 Jun 30. Stroke. 2022. PMID: 35770672
-
Rescue stenting after the failure of mechanical thrombectomy to treat acute intracranial atherosclerotic occlusion.Front Neurol. 2023 Jan 10;13:1001496. doi: 10.3389/fneur.2022.1001496. eCollection 2022. Front Neurol. 2023. PMID: 36703624 Free PMC article.
-
Rescue Stenting for Failed Mechanical Thrombectomy in Acute Ischemic Stroke: A Multicenter Experience.Stroke. 2018 Apr;49(4):958-964. doi: 10.1161/STROKEAHA.117.020072. Epub 2018 Mar 16. Stroke. 2018. PMID: 29581342
-
Outcomes of Patients With Atrial Fibrillation Following Thrombectomy for Stroke: A Systematic Review and Meta-analysis.JAMA Netw Open. 2023 Jan 3;6(1):e2249993. doi: 10.1001/jamanetworkopen.2022.49993. JAMA Netw Open. 2023. PMID: 36607633 Free PMC article.
Cited by
-
Rescue stenting after failed mechanical thrombectomy: The RES-CAT study.Eur Stroke J. 2025 Jan 2:23969873241308680. doi: 10.1177/23969873241308680. Online ahead of print. Eur Stroke J. 2025. PMID: 39745051 Free PMC article.
-
Determinants of day-1 stent patency following rescue intracranial stenting in failed intracranial thrombectomy.Interv Neuroradiol. 2025 May 21:15910199251339900. doi: 10.1177/15910199251339900. Online ahead of print. Interv Neuroradiol. 2025. PMID: 40398455 Free PMC article.
-
First-in-human trial of a self-expandable, temporary dilation system for intracranial atherosclerotic disease in patients presenting with acute ischemic stroke.J Neurointerv Surg. 2024 Nov 22;16(12):1232-1236. doi: 10.1136/jnis-2023-020983. J Neurointerv Surg. 2024. PMID: 38041666 Free PMC article. Clinical Trial.
-
Comparison of early versus late rescue stenting after failed thrombectomy for intracranial atherosclerosis-related large vessel occlusion.Acta Neurochir (Wien). 2025 Feb 25;167(1):54. doi: 10.1007/s00701-025-06470-2. Acta Neurochir (Wien). 2025. PMID: 40000453 Free PMC article.
-
Is intraprocedural intravenous aspirin safe for patients who require emergent extracranial stenting during mechanical thrombectomy?Stroke Vasc Neurol. 2024 Jun 21;9(3):279-288. doi: 10.1136/svn-2022-002267. Stroke Vasc Neurol. 2024. PMID: 37788913 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials