

Laparoscopic versus open pancreaticoduodenectomy for pancreatic and periampullary tumor: A meta-analysis of randomized controlled trials and non-randomized comparative studies
- PMID: 36761416
- PMCID: PMC9905842
- DOI: 10.3389/fonc.2022.1093395
Laparoscopic versus open pancreaticoduodenectomy for pancreatic and periampullary tumor: A meta-analysis of randomized controlled trials and non-randomized comparative studies
Abstract
Objective: This meta-analysis compares the perioperative outcomes of laparoscopic pancreaticoduodenectomy (LPD) to those of open pancreaticoduodenectomy (OPD) for pancreatic and periampullary tumors.
Background: LPD has been increasingly applied in the treatment of pancreatic and periampullary tumors. However, the perioperative outcomes of LPD versus OPD are still controversial.
Methods: PubMed, Web of Science, EMBASE, and the Cochrane Library were searched to identify randomized controlled trials (RCTs) and non-randomized comparative trials (NRCTs) comparing LPD versus OPD for pancreatic and periampullary tumors. The main outcomes were mortality, morbidity, serious complications, and hospital stay. The secondary outcomes were operative time, blood loss, transfusion, postoperative pancreatic fistula (POPF), postpancreatectomy hemorrhage (PPH), bile leak (BL), delayed gastric emptying (DGE), lymph nodes harvested, R0 resection, reoperation, and readmission. RCTs were evaluated by the Cochrane risk-of-bias tool. NRCTs were assessed using a modified tool from the Methodological Index for Non-randomized Studies. Data were pooled as odds ratio (OR) or mean difference (MD). This study was registered at PROSPERO (CRD42022338832).
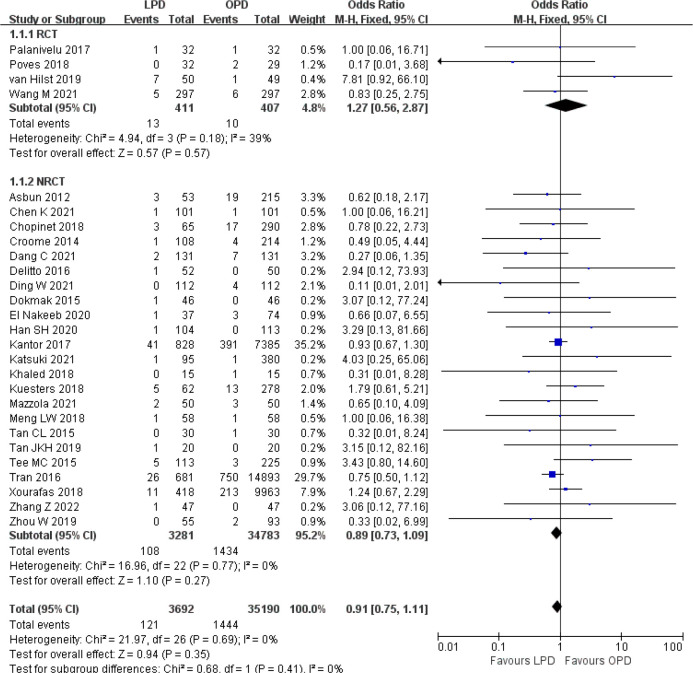
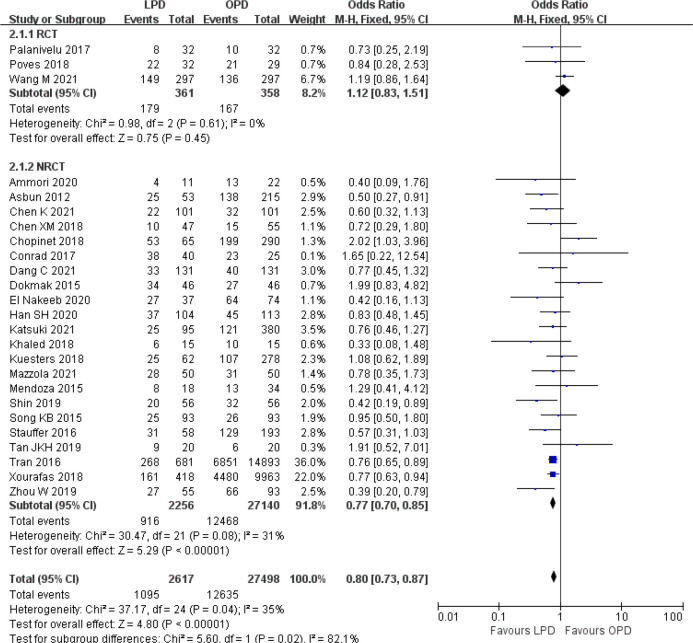
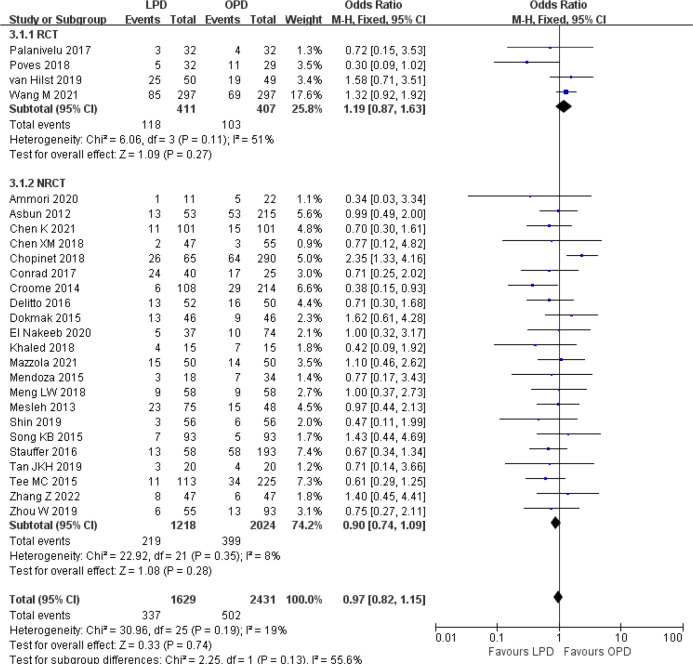
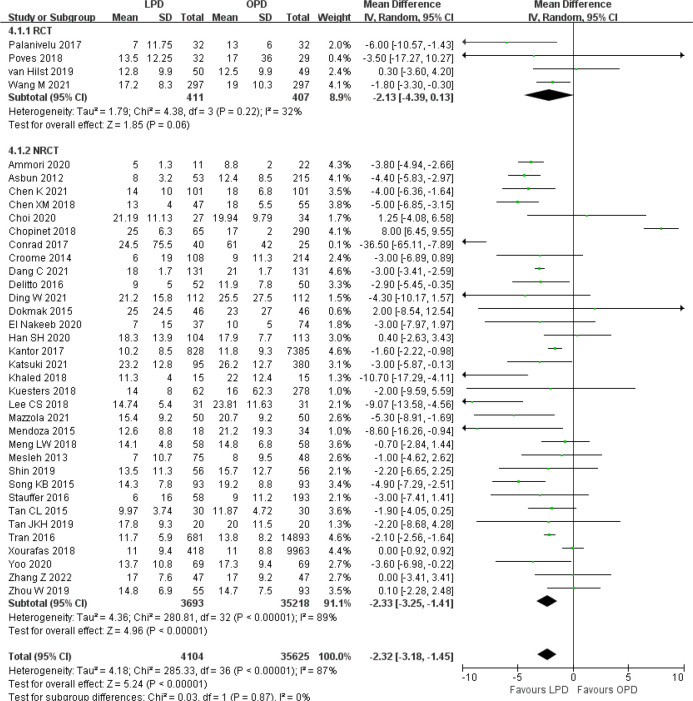
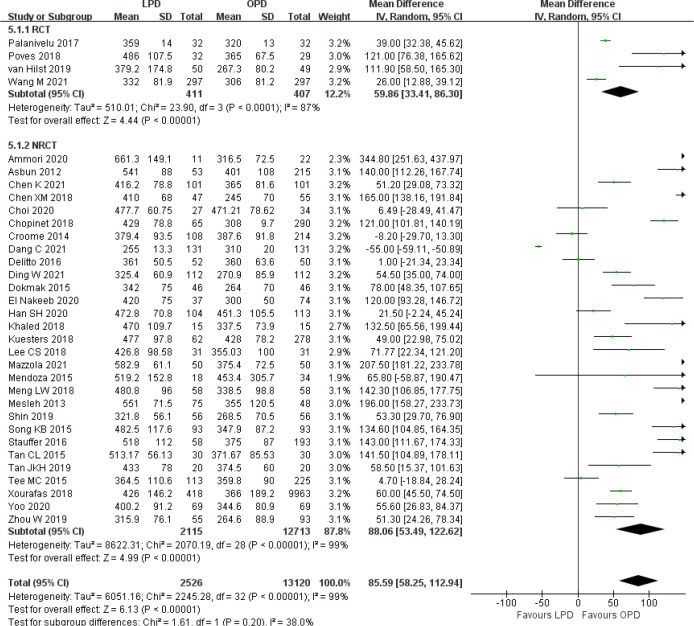
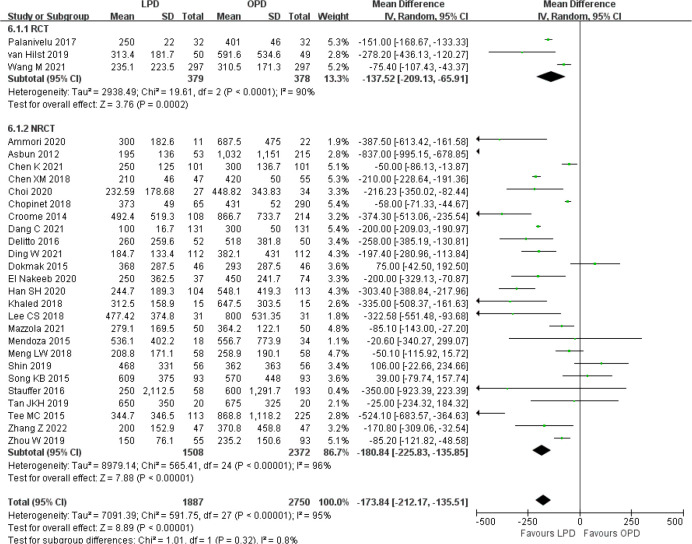
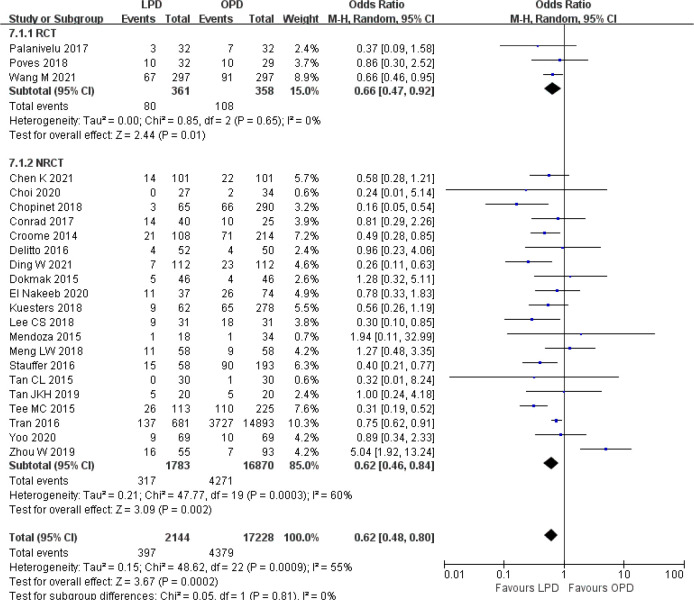
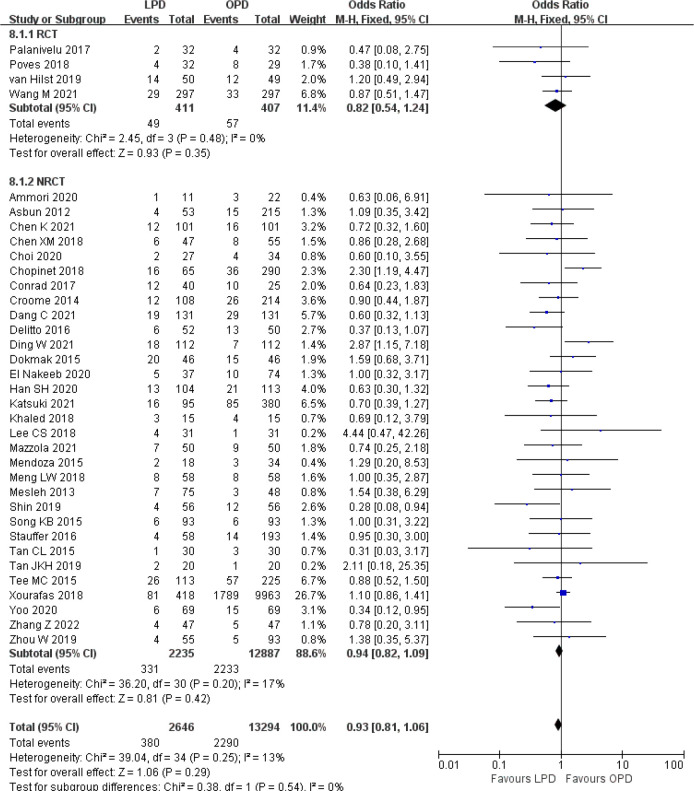
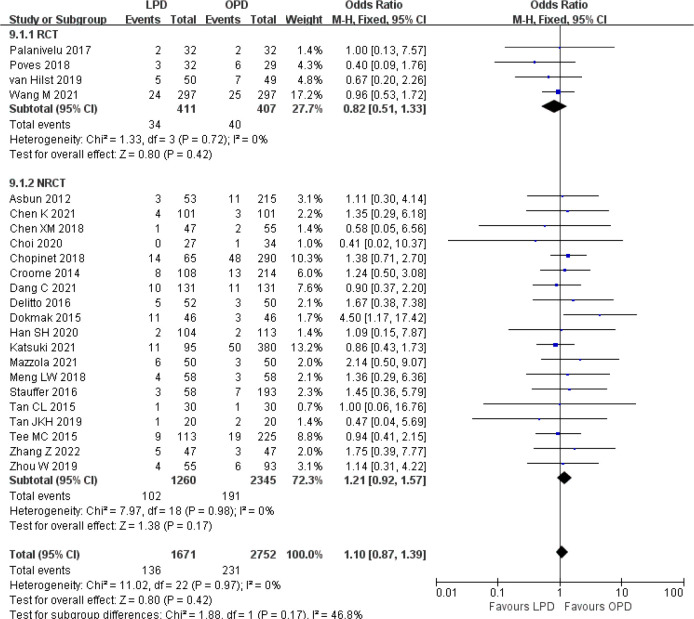
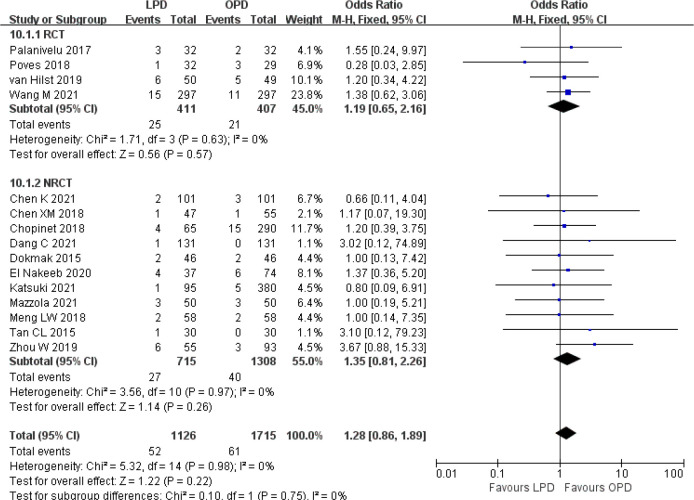
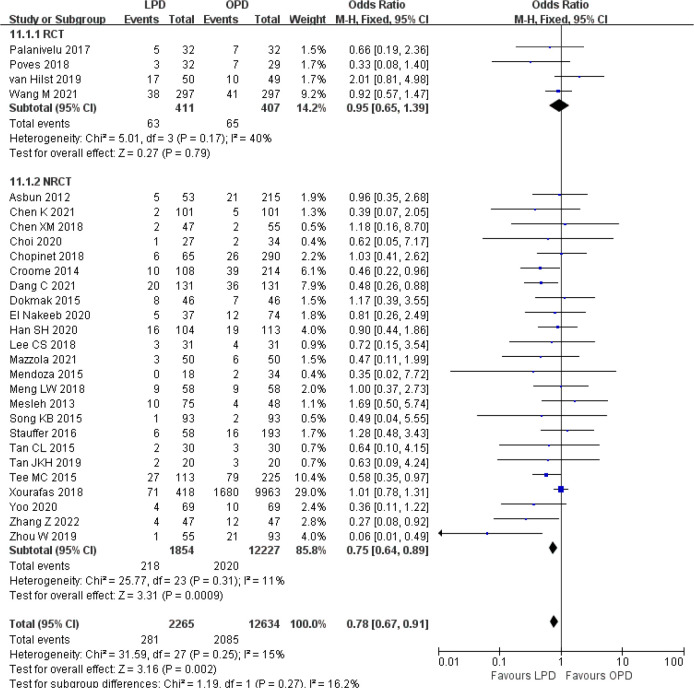
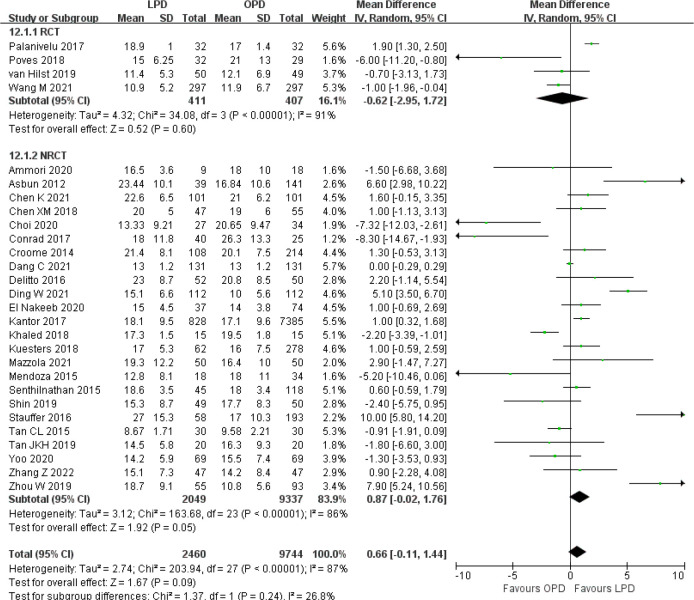
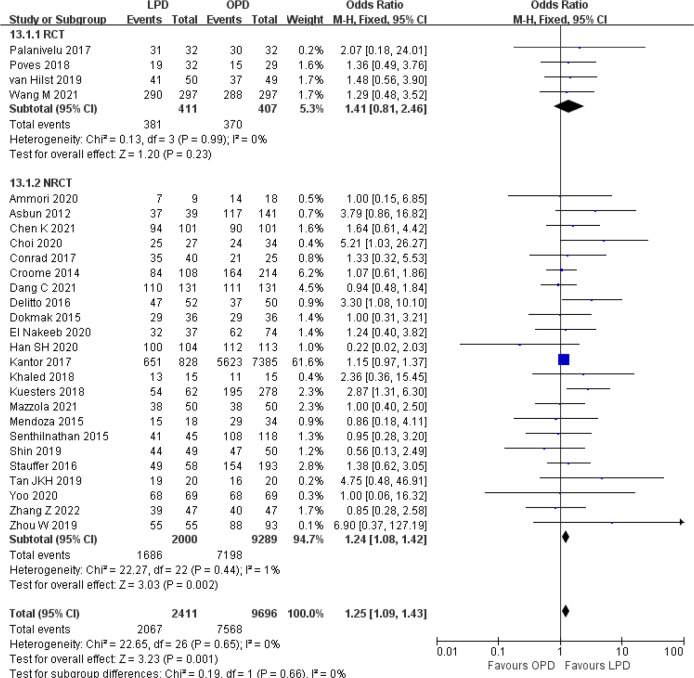
Results: Four RCTs and 35 NRCTs concerning a total of 40,230 patients (4,262 LPD and 35,968 OPD) were included. Meta-analyses showed no significant differences in mortality (OR 0.91, p = 0.35), serious complications (OR 0.97, p = 0.74), POPF (OR 0.93, p = 0.29), PPH (OR 1.10, p = 0.42), BL (OR 1.28, p = 0.22), harvested lymph nodes (MD 0.66, p = 0.09), reoperation (OR 1.10, p = 0.41), and readmission (OR 0.95, p = 0.46) between LPD and OPD. Operative time was significantly longer for LPD (MD 85.59 min, p < 0.00001), whereas overall morbidity (OR 0.80, p < 0.00001), hospital stay (MD -2.32 days, p < 0.00001), blood loss (MD -173.84 ml, p < 0.00001), transfusion (OR 0.62, p = 0.0002), and DGE (OR 0.78, p = 0.002) were reduced for LPD. The R0 rate was higher for LPD (OR 1.25, p = 0.001).
Conclusions: LPD is associated with non-inferior short-term surgical outcomes and oncologic adequacy compared to OPD when performed by experienced surgeons at large centers. LPD may result in reduced overall morbidity, blood loss, transfusion, and DGE, but longer operative time. Further RCTs should address the potential advantages of LPD over OPD.
Systematic review registration: PROSPERO, identifier CRD42022338832.
Keywords: laparoscopic pancreaticoduodenectomy; meta-analysis; open pancreaticoduodenectomy; pancreatic head; periampullary tumor; whipple.
Copyright © 2023 Yan, Hua, Chang, Zhu, Sha and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Laparoscopic Versus Open Pancreaticoduodenectomy: A Systematic Review and Meta-analysis of Randomized Controlled Trials.Ann Surg. 2020 Jan;271(1):54-66. doi: 10.1097/SLA.0000000000003309. Ann Surg. 2020. PMID: 30973388
-
Perioperative and short-term oncological outcomes following laparoscopic versus open pancreaticoduodenectomy after learning curve in the past 10 years: a systematic review and meta-analysis.Gland Surg. 2021 May;10(5):1655-1668. doi: 10.21037/gs-20-916. Gland Surg. 2021. PMID: 34164310 Free PMC article.
-
Laparoscopic vs. Open Pancreaticoduodenectomy After Learning Curve: A Systematic Review and Meta-Analysis of Single-Center Studies.Front Surg. 2021 Sep 10;8:715083. doi: 10.3389/fsurg.2021.715083. eCollection 2021. Front Surg. 2021. Retraction in: Front Surg. 2022 Jul 26;9:988654. doi: 10.3389/fsurg.2022.988654. PMID: 34568416 Free PMC article. Retracted.
-
Laparoscopic Pancreaticoduodenectomy Versus Conventional Open Approach for Patients With Pancreatic Duct Adenocarcinoma: An Up-to-Date Systematic Review and Meta-Analysis.Front Oncol. 2021 Oct 27;11:749140. doi: 10.3389/fonc.2021.749140. eCollection 2021. Front Oncol. 2021. PMID: 34778064 Free PMC article.
-
Robotic versus laparoscopic pancreaticoduodenectomy for pancreatic and periampullary tumors: a meta-analysis.Front Oncol. 2024 Nov 19;14:1486504. doi: 10.3389/fonc.2024.1486504. eCollection 2024. Front Oncol. 2024. PMID: 39629002 Free PMC article.
Cited by
-
The state of robotic vs. open pancreatoduodenectomy.Gland Surg. 2024 Aug 31;13(8):1344-1348. doi: 10.21037/gs-24-182. Epub 2024 Aug 20. Gland Surg. 2024. PMID: 39282045 Free PMC article. No abstract available.
-
Short-term surgical outcomes of open, laparoscopic, and robot-assisted pancreatoduodenectomy: A comparative, single-center, retrospective study.Asian J Endosc Surg. 2025 Jan-Dec;18(1):e13397. doi: 10.1111/ases.13397. Asian J Endosc Surg. 2025. PMID: 39428321 Free PMC article.
-
Comparison of short-term outcomes of robotic versus open pancreaticoduodenectomy: a meta-analysis of randomized controlled trials and propensity-score-matched studies.Int J Surg. 2025 Jan 1;111(1):1214-1230. doi: 10.1097/JS9.0000000000001871. Int J Surg. 2025. PMID: 38935118 Free PMC article.
-
Editorial: Technological innovations and pancreatic cancer.Front Oncol. 2024 Oct 7;14:1497367. doi: 10.3389/fonc.2024.1497367. eCollection 2024. Front Oncol. 2024. PMID: 39435295 Free PMC article. No abstract available.
-
Exploring the landscape of minimally invasive pancreatic surgery: Progress, challenges, and future directions.World J Gastrointest Surg. 2024 Oct 27;16(10):3094-3103. doi: 10.4240/wjgs.v16.i10.3094. World J Gastrointest Surg. 2024. PMID: 39575294 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources