

More recent insights into the breast cancer burden across BRICS-Plus: Health consequences in key nations with emerging economies using the global burden of disease study 2019
- PMID: 36761973
- PMCID: PMC9902930
- DOI: 10.3389/fonc.2023.1100300
More recent insights into the breast cancer burden across BRICS-Plus: Health consequences in key nations with emerging economies using the global burden of disease study 2019
Abstract
Background: Brazil, Russia, India, China, South Africa, and 30 other Asian nations make up the BRICS-Plus, a group of developing countries that account for about half of the world's population and contribute significantly to the global illness burden. This study aimed to analyzed the epidemiological burden of female breast cancer (BC) across the BRICS-Plus from 1990 to 2019 and studied the associations with age, period, birth cohort and countries' sociodemographic index (SDI).
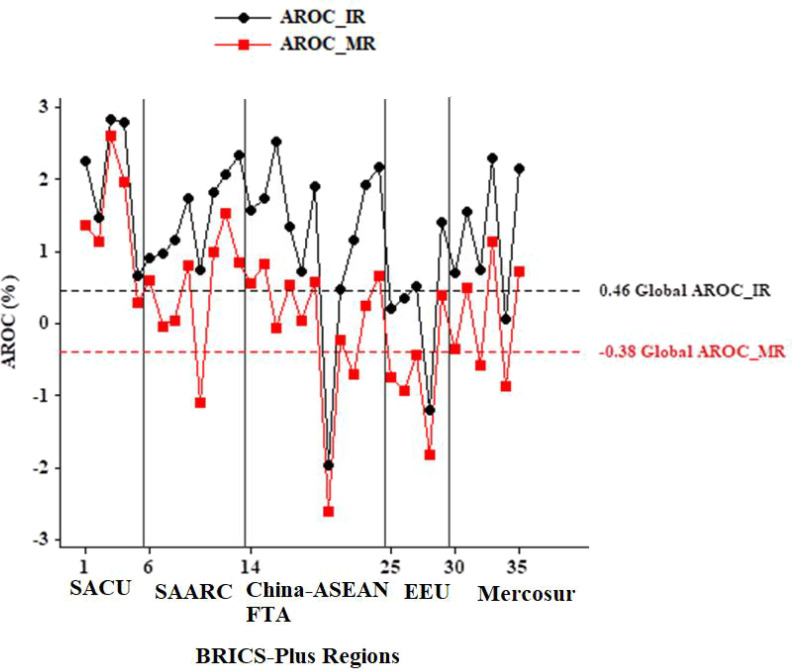
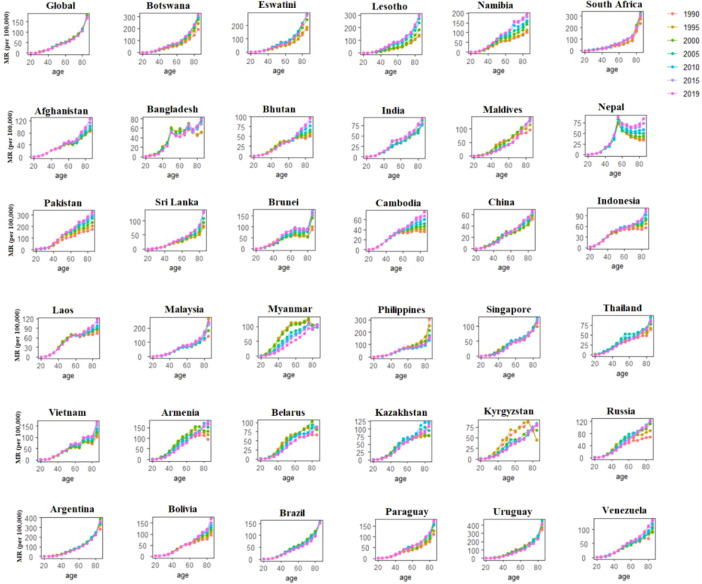
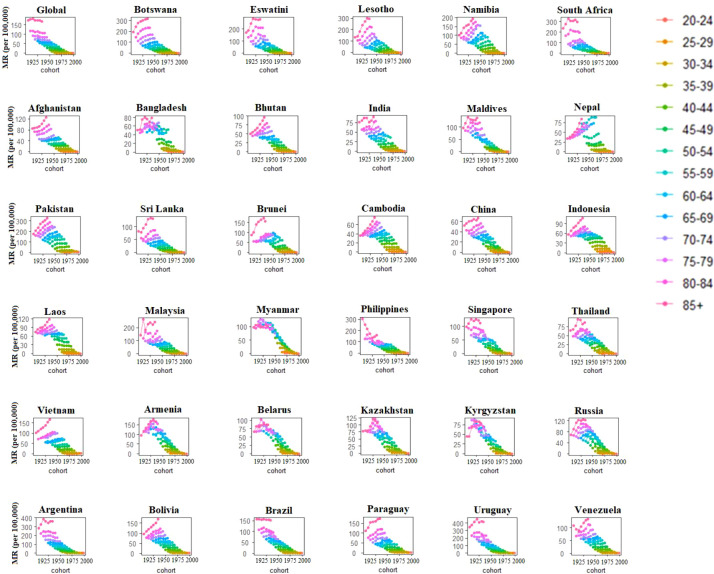
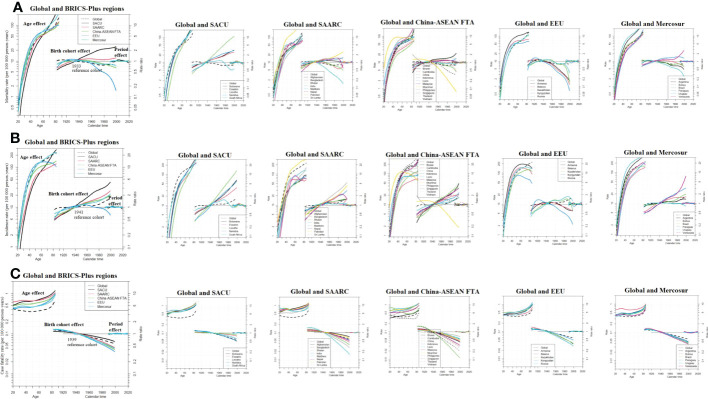
Methods: The BC mortality and incidence estimates came from the 2019 Global Burden of Disease Study. We estimated cohort and period effects in BC outcomes between 1990 and 2019 using age-period-cohort (APC) modeling. The maximum likelihood (ML) of the APC-model Poisson with log (Y) based on the natural-spline function was used to estimate the rate ratio (RR). We used annualized rate of change (AROC) to quantify change over the previous 30 years in BC across BRICS-Plus and compare it to the global.
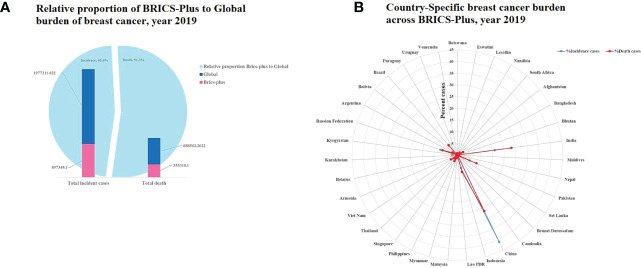
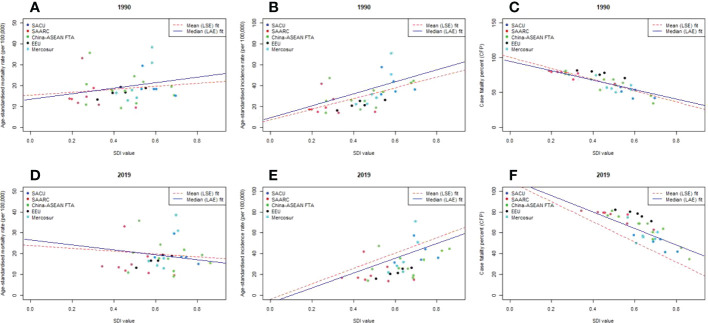
Results: In 2019, there were about 1.98 million female BC cases (age-standardized rate of 45.86 [95% UI: 41.91, 49.76]) and 0.69 million deaths (age-standardized rate of 15.88 [95% UI: 14.66, 17.07]) around the globe. Among them, 45.4% of incident cases and 51.3% of deaths were attributed to the BRICS-Plus. China (41.1% cases and 26.5% deaths) and India (16.1% cases and 23.1% deaths) had the largest proportion of incident cases and deaths among the BRICS-Plus nations in 2019. Pakistan came in third with 5.6% cases and 8.8% deaths. Over the past three decades, from 1990 to 2019, the BRICS-Plus region's greatest AROC was seen in Lesotho (2.61%; 95%UI: 1.99-2.99). The birth cohort impacts on BC vary significantly among the BRICS-Plus nations. Overall, the risk of case-fatality rate tended to decline in all BRICS-Plus nations, notably in South Asian Association for Regional Cooperation (SAARC) and China-ASEAN Free Trade Area (China-ASEAN FTA) countries, and the drop in risk in the most recent cohort was lowest in China and the Maldives. Additionally, there was a substantial negative link between SDI and case fatality rate (r1990= -0.91, p<0.001; r2019= -0.89, p<0.001) in the BRICS-Plus in both 1990 and 2019, with the Eurasian Economic Union (EEU) nations having the highest case fatality rate.
Conclusions: The BC burden varies remarkably between different BRICS-Plus regions. Although the BRICS' efforts to regulate BC succeeded, the overall improvements lagged behind those in high-income Asia-Pacific nations. Every BRICS-Plus country should strengthen specific public health approaches and policies directed at different priority groups, according to BRIC-Plus and other high-burden nations.
Keywords: APC; BRICS-Plus; SDI; breast cancer; case fatality; mortality.
Copyright © 2023 Mubarik, Luo, Iqbal, Nawsherwan, Bai and Yu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Breast cancer epidemiology and sociodemographic differences in BRICS-plus countries from 1990 to 2019: An age period cohort analysis.SSM Popul Health. 2023 Apr 29;22:101418. doi: 10.1016/j.ssmph.2023.101418. eCollection 2023 Jun. SSM Popul Health. 2023. PMID: 37215157 Free PMC article.
-
Estimating disparities of prostate cancer burden and its attributable risk factors for males across the BRICS-plus, 1990-2019: A comparable study of key nations with emerging economies.Prostate. 2024 May;84(6):570-583. doi: 10.1002/pros.24673. Epub 2024 Feb 8. Prostate. 2024. PMID: 38328967
-
Time Trends in Cardiovascular Disease Mortality Across the BRICS: An Age-Period-Cohort Analysis of Key Nations With Emerging Economies Using the Global Burden of Disease Study 2017.Circulation. 2020 Mar 10;141(10):790-799. doi: 10.1161/CIRCULATIONAHA.119.042864. Epub 2020 Jan 16. Circulation. 2020. PMID: 31941371
-
Waste electrical and electronic equipment management and Basel Convention compliance in Brazil, Russia, India, China and South Africa (BRICS) nations.Waste Manag Res. 2016 Aug;34(8):693-707. doi: 10.1177/0734242X16652956. Epub 2016 Jul 15. Waste Manag Res. 2016. PMID: 27422616 Review.
-
The priority areas and possible pathways for health cooperation in BRICS countries.Glob Health Res Policy. 2023 Aug 28;8(1):36. doi: 10.1186/s41256-023-00318-x. Glob Health Res Policy. 2023. PMID: 37641146 Free PMC article. Review.
Cited by
-
Estimating disparities in breast cancer screening programs towards mortality, case fatality, and DALYs across BRICS-plus.BMC Med. 2023 Sep 1;21(1):299. doi: 10.1186/s12916-023-03004-4. BMC Med. 2023. PMID: 37653535 Free PMC article.
-
Regional differences in the disease burden and attributable risk factors of female cancers.Sci Rep. 2025 Apr 16;15(1):13092. doi: 10.1038/s41598-025-97482-6. Sci Rep. 2025. PMID: 40240430 Free PMC article.
-
A comparative study of incidence, mortality and disability adjusted life years (DALYs) for leading cancers in BRICS countries.Ecancermedicalscience. 2024 Sep 19;18:1773. doi: 10.3332/ecancer.2024.1773. eCollection 2024. Ecancermedicalscience. 2024. PMID: 39430096 Free PMC article. Review.
-
Historical trends of breast cancer burden attributable to metabolic factors among Chinese women, 1990-2019: A population-based epidemiological study.Thorac Cancer. 2024 Jun;15(16):1279-1286. doi: 10.1111/1759-7714.15316. Epub 2024 Apr 25. Thorac Cancer. 2024. PMID: 38664975 Free PMC article.
-
Dataset of obesity in relation to female-specific cancers in middle eastern countries, 1990 to 2016.BMC Res Notes. 2025 Mar 25;18(1):124. doi: 10.1186/s13104-025-07187-2. BMC Res Notes. 2025. PMID: 40134010 Free PMC article.
References
-
- Li N, Deng Y, Zhou L, Tian T, Yang S, Wu Y, et al. . Global burden of breast cancer and attributable risk factors in 195 countries and territories, from 1990 to 2017: results from the global burden of disease study 2017. J Hematol Oncol (2019) 12(1):140. doi: 10.1186/s13045-019-0700-2 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous