

Long-term outcomes of laparoscopic liver resection versus open liver resection for hepatocellular carcinoma: A single-center 10-year experience
- PMID: 36761978
- PMCID: PMC9905741
- DOI: 10.3389/fonc.2023.1112380
Long-term outcomes of laparoscopic liver resection versus open liver resection for hepatocellular carcinoma: A single-center 10-year experience
Abstract
Background: Laparoscopic liver resection (LLR) for hepatocellular carcinoma (HCC) has increased. However, the long-term outcomes of LLR for HCCs should be validated further. Besides, the validity of laparoscopic minor liver resection in difficult segments (1, 4a, 7, 8) (LMLR-DS) and laparoscopic major hepatectomy (LMH) for HCCs need to be studied.
Methods: A total of 1773 HCC patients were collected: 683 received LLR and 1090 received OLR. Propensity score matching (PSM) with 1:1 ratio was used to eliminate the selection bias. Short-term and long-term outcomes were compared. In subgroup analyses, the validity of LMLR-DS or LMH for HCCs was studied.
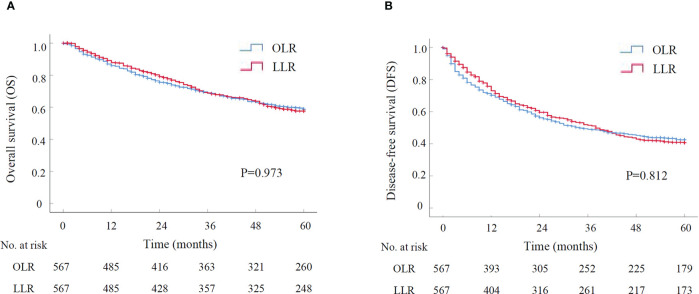
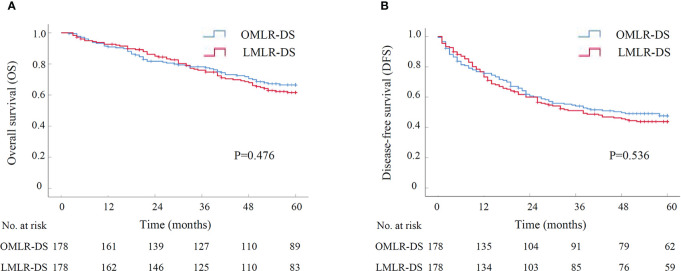
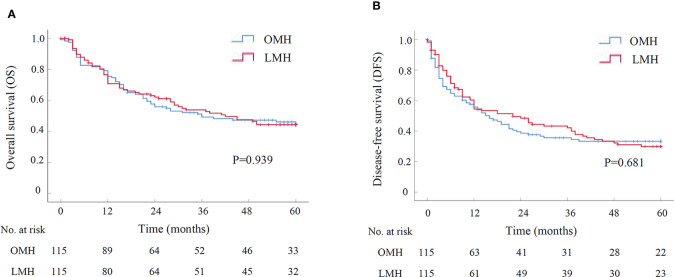
Results: After PSM, 567 patients were in LLR or OLR group. LLR had lower intraoperative blood-loss and shorter postoperative hospital-stays than OLR. The postoperative complications were lower in LLR group (23.8% vs. 32.8%, P=0.001). The Overall survival (OS) and disease-free survival (DFS) had no significant difference between LLR and OLR groups (P=0.973, P=0.812). The cumulative 1-, 3-, and 5-year OR rates were 87.9%, 68.9%, and 57.7% for LLR group, and 85.9%, 68.8%, 58.8% for OLR group. The cumulative 1-, 3-, and 5-year DFS rates were 73.0%, 51.5%, 40.6% for LLR group, and 70.3%, 49.0%, 42.4% for OLR group. In subgroup analyses, 178 patients were in LMLR-DS or open surgery (OMLR-DS) group after PSM. LMLR-DS had lower intraoperative blood-loss and shorter postoperative hospital-stays than OMLR-DS. The postoperative complications were lower in LMLR-DS group. The OS and DFS had no difference between LMLR-DS and OMLR-DS groups. The cumulative 5-year OR and DFS rates were 61.6%, 43.9% for LMLR-DS group, and 66.5%, 47.7% for OMLR-DS group. In another subgroup analyses, 115 patients were in LMH or open major hepatectomy (OMH) group. LMH had lower blood-loss and shorter postoperative hospital-stays than OMH. The complications, OS and DFS had no significantly differences between two groups. The cumulative 5-year OR and DFS rates were 44.3%, 29.9% for LMH group, and 44.7%, 33.2% for OMH group.
Conclusions: LLR for HCCs showed better short-term outcomes and comparable long-term outcomes with OLR, even for patients who received LMLR-DS or LMH. LLR could be reliable and recommended for HCC treatment.
Keywords: hepatocellar carcinoma; laparoscopic liver resection; laparoscopic major hepatectomy; laparoscopic minor liver resection in difficult segments; open liver resection; prognosis.
Copyright © 2023 Tian, Leng, Chen, Cao, Cao, Wang, Li, Wang, Zheng and Li.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Laparoscopic versus open major liver resection for hepatocellular carcinoma: systematic review and meta-analysis of comparative cohort studies.BMC Cancer. 2019 Nov 6;19(1):1047. doi: 10.1186/s12885-019-6240-x. BMC Cancer. 2019. PMID: 31694596 Free PMC article.
-
Long-term perioperative outcomes of pure laparoscopic liver resection versus open liver resection for hepatocellular carcinoma: a retrospective study.Surg Endosc. 2020 Feb;34(2):796-805. doi: 10.1007/s00464-019-06831-w. Epub 2019 Jun 3. Surg Endosc. 2020. PMID: 31161292
-
Perioperative and long-term survival outcomes of laparoscopic versus open hepatectomy for BCLC stage A large hepatocellular carcinoma patients in difficult segments: A two-centre, propensity score matching analysis.Front Oncol. 2023 Mar 10;13:1095357. doi: 10.3389/fonc.2023.1095357. eCollection 2023. Front Oncol. 2023. PMID: 36969010 Free PMC article.
-
Minor laparoscopic liver resection for Hepatocellular Carcinoma is safer than minor open resection, especially for less compensated cirrhotic patients: Propensity score analysis.Surg Oncol. 2018 Dec;27(4):722-729. doi: 10.1016/j.suronc.2018.10.001. Epub 2018 Oct 3. Surg Oncol. 2018. PMID: 30449499
-
Laparoscopic versus open liver resection for hepatocellular carcinoma in elderly patients: A systematic review and meta-analysis of propensity score-matched studies.Front Oncol. 2022 Nov 14;12:939877. doi: 10.3389/fonc.2022.939877. eCollection 2022. Front Oncol. 2022. PMID: 36452485 Free PMC article.
Cited by
-
Safety and Perioperative Outcomes of Laparoscopic vs. Open Hepatectomy of Central-Located Liver Lesions: A Multicenter, Propensity Score-Matched, Retrospective Cohort Study.J Clin Med. 2023 Mar 10;12(6):2164. doi: 10.3390/jcm12062164. J Clin Med. 2023. PMID: 36983169 Free PMC article.
-
Combined Bone Mineral Density (BMD) and Monocyte-to-Lymphocyte Ratio (MLR) Predicts Recurrence and Prognosis in Hepatocellular Carcinoma Patients Following Liver Resection.Risk Manag Healthc Policy. 2024 Nov 9;17:2741-2754. doi: 10.2147/RMHP.S473247. eCollection 2024. Risk Manag Healthc Policy. 2024. PMID: 39539485 Free PMC article.
-
Incidence of incisional hernia following liver surgery for colorectal liver metastases. Does the laparoscopic approach reduce the risk? A comparative study.Ann Hepatobiliary Pancreat Surg. 2024 May 31;28(2):155-160. doi: 10.14701/ahbps.23-138. Epub 2024 Mar 4. Ann Hepatobiliary Pancreat Surg. 2024. PMID: 38433531 Free PMC article.
-
Laparoscopic counterclockwise modular mesohepatectomy for hepatocellular carcinoma: a standardized anatomical approach (with video).Front Oncol. 2025 Jun 18;15:1599403. doi: 10.3389/fonc.2025.1599403. eCollection 2025. Front Oncol. 2025. PMID: 40606974 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous