

Novel description on esophageal timed barium swallow: a correlation between advanced parametrization and esophageal X-ray images
- PMID: 36762225
- PMCID: PMC9876766
- DOI: 10.22037/ghfbb.v15i4.2467
Novel description on esophageal timed barium swallow: a correlation between advanced parametrization and esophageal X-ray images
Abstract
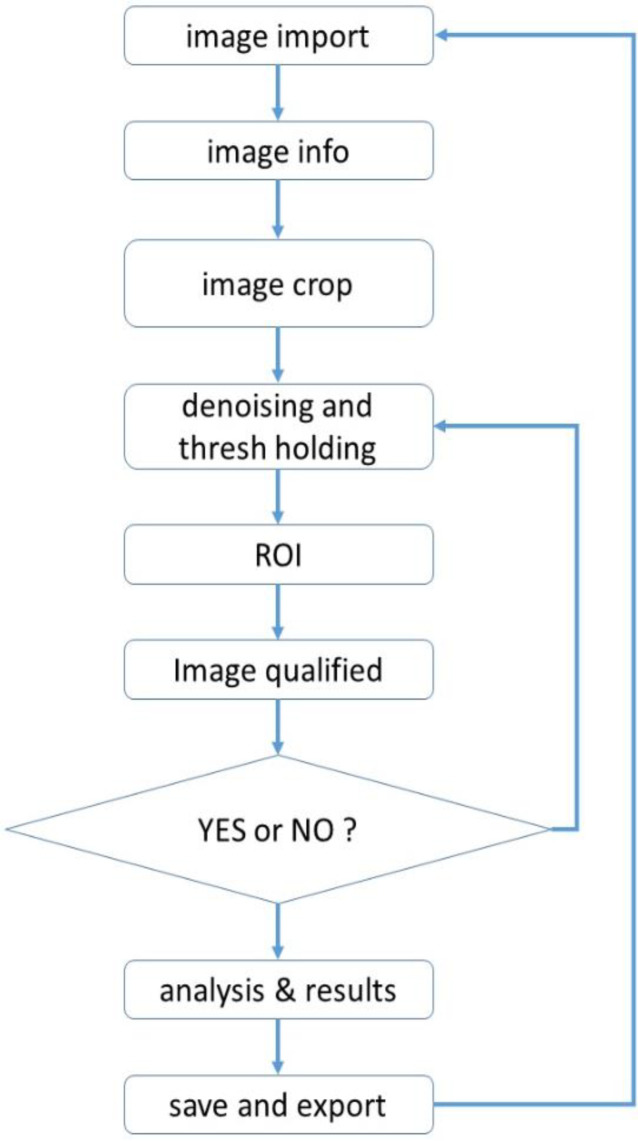
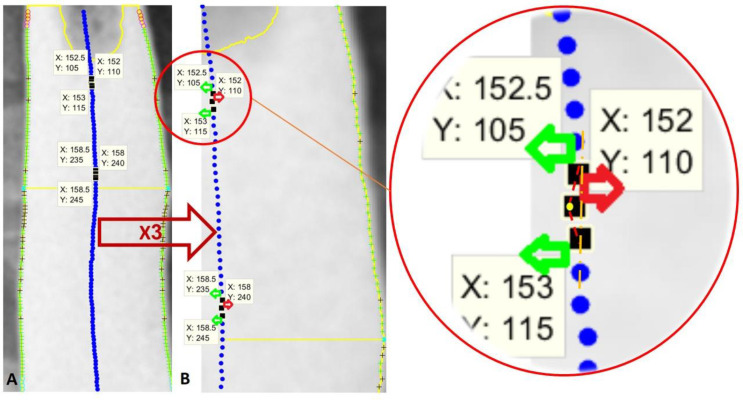
Aim: The TBS-derived image processing method, based on the observer's diagnosis, has been developed in the current investigation. Image parametrization is proposed for both novel description and convergent shreds of evidence.
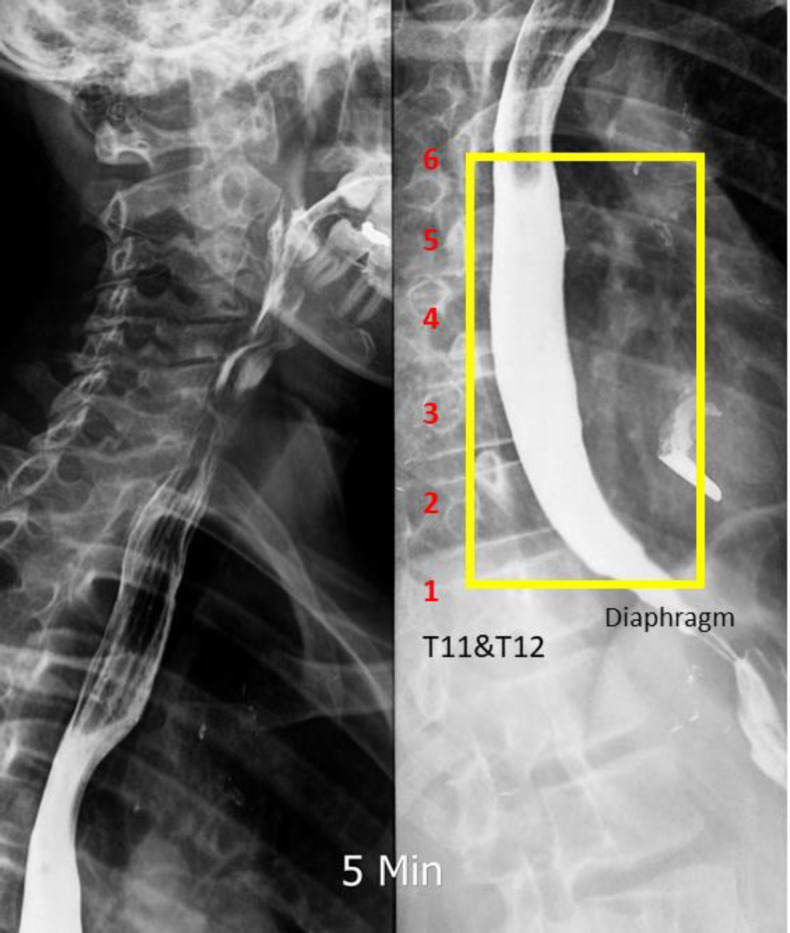
Background: Condensed X-ray images of the esophageal timed barium swallow (TBS) provide substantial implications for elucidating the pathophysiological dimensions of esophageal motility disorders.
Methods: Through the simultaneous study on TBS and high-resolution manometry (HRM) findings, we performed a retrospective cohort study on 252 patients from March 2018 to October 2019. Interventions, irrelevant information, and insufficient patient data were excluded. Only subjects with adequate data and acceptable test accuracy were considered for participation. We reviewed 117 Dicom (digital imaging and communications in medicine) X-ray images from patients with confirmed diagnoses of achalasia type II, esophagogastric junction outflow obstruction (EGJOO), or non-achalasia.
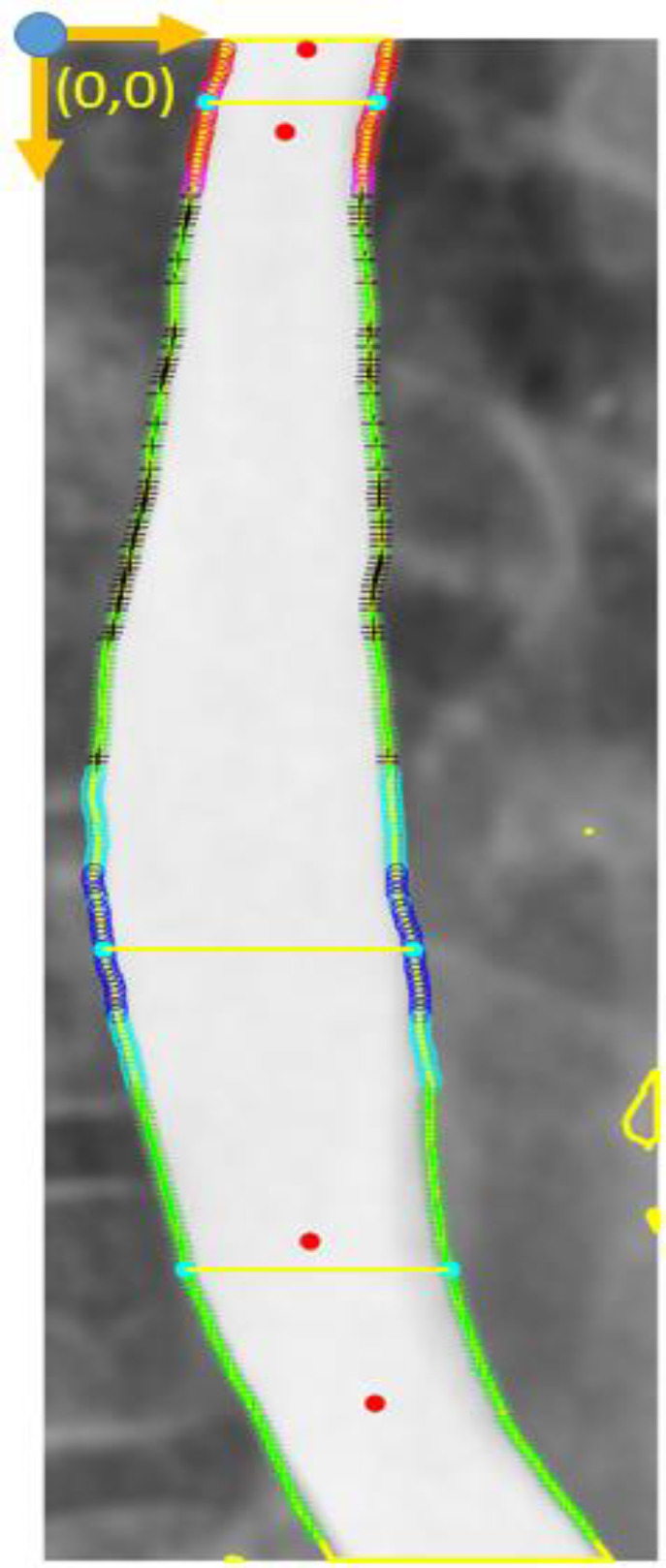
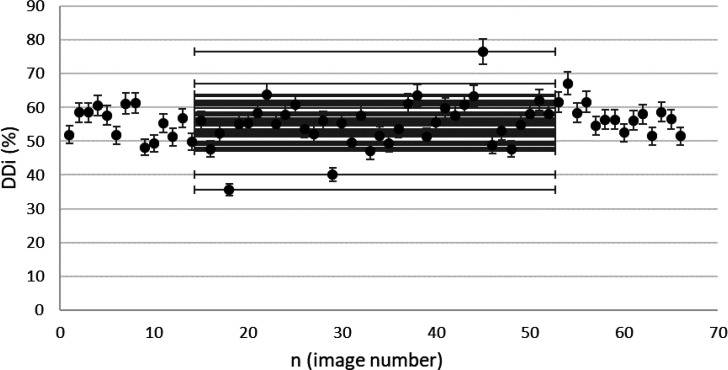
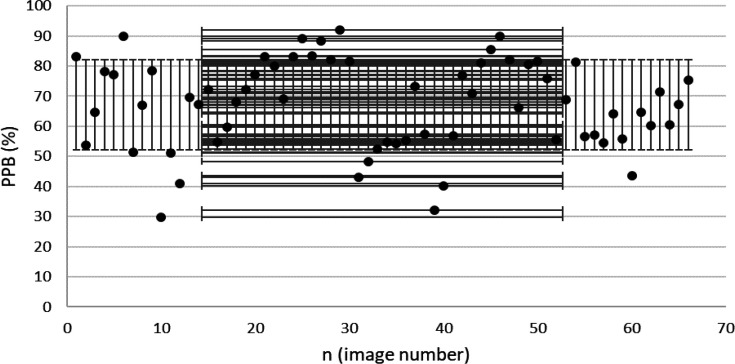
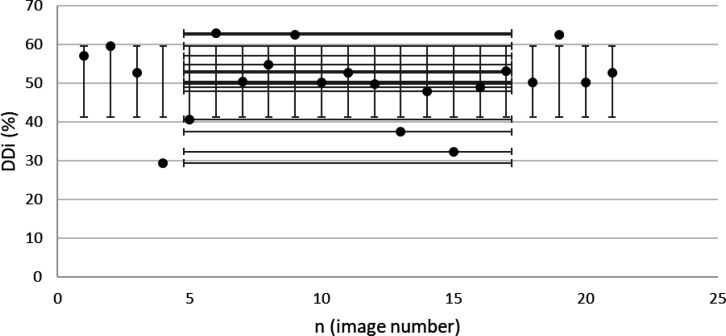
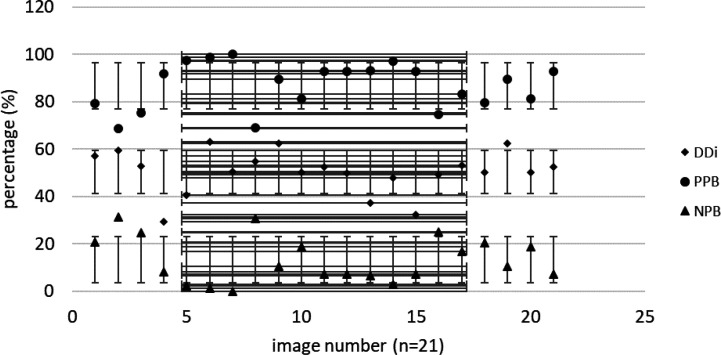
Results: The results suggested a cut-off level of 47% in DDi (dilated diameter index) as a sign of the dilated body. In achalasia type II patients (n=66 images), the mean DDi was 55.6%. Our method presented a sensitivity of 95% and a specificity of 93% compared to images of the non-achalasia findings. The mean DDi in EGJOO patients was 50.4%, according to the 27 images. Moreover, results from EGJOO patients provided a sensitivity of 85% and specificity of 87%.
Conclusion: TBS is an efficacious method and a prominent component in the process of achalasia diagnosis. Standard parametrization might develop radiological exports proposed by DDi. Our method could assist in obtaining a non-invasive medical diagnosis and help advance diagnostic reports to identify achalasia subtypes somewhat earlier. To the best of our knowledge, this interface is an innovative parametrization for TBS image review.
Keywords: Achalasia; Esophageal barium time swallow; High-resolution esophageal manometry; Image processing.
Conflict of interest statement
The authors declare that there is no conflict of interests.
Figures
Similar articles
-
Timed Barium Swallow: Diagnostic Role and Predictive Value in Untreated Achalasia, Esophagogastric Junction Outflow Obstruction, and Non-Achalasia Dysphagia.Am J Gastroenterol. 2018 Feb;113(2):196-203. doi: 10.1038/ajg.2017.370. Epub 2017 Dec 19. Am J Gastroenterol. 2018. PMID: 29257145
-
Timed barium swallow: Esophageal stasis varies markedly across subtypes of esophagogastric junction obstruction.Neurogastroenterol Motil. 2022 Mar;34(3):e14322. doi: 10.1111/nmo.14322. Epub 2022 Jan 24. Neurogastroenterol Motil. 2022. PMID: 35072303
-
[TIMED BARIUM SWALLOW: CLINICAL UTILITY, INDICATIONS AND HOW TO INTERPRET THE STUDY].Harefuah. 2025 Feb;164(2):108-113. Harefuah. 2025. PMID: 39987480 Review. Hebrew.
-
How to effectively use and interpret the barium swallow: Current role in esophageal dysphagia.Neurogastroenterol Motil. 2023 Oct;35(10):e14605. doi: 10.1111/nmo.14605. Epub 2023 Apr 27. Neurogastroenterol Motil. 2023. PMID: 37103465 Review.
-
Optimal cutoff value of integrated relaxation pressure on the esophagogastric junction to detect outflow obstruction using starlet high-resolution manometry system.J Gastroenterol. 2021 Mar;56(3):231-239. doi: 10.1007/s00535-020-01757-w. Epub 2021 Jan 9. J Gastroenterol. 2021. PMID: 33423114
Cited by
-
Modern Achalasia: Diagnosis, Classification, and Treatment.J Neurogastroenterol Motil. 2023 Oct 30;29(4):419-427. doi: 10.5056/jnm23125. J Neurogastroenterol Motil. 2023. PMID: 37814432 Free PMC article. Review.
References
-
- Malagelada JR, Bazzoli F, Boeckxstaens G, De Looze D, Fried M, Kahrilas P, et al. World gastroenterology organisation global guidelines: dysphagia--global guidelines and cascades update September 2014. J Clin Gastroenterol. 2015;49:370–8. - PubMed
-
- Gasiorowska A. Fass R Current approach to dysphagia. Gastroenterol Hepatol. 2009;5:269–279.
-
- Vantrappen G, Janssens J, Hellemans J, Coremans G. Achalasia, diffuse esophageal spasm, and related motility disorders. Gastroenterology. 1979;76:450–457. - PubMed
LinkOut - more resources
Full Text Sources