

Surgery After BRAF-Directed Therapy Is Associated with Improved Survival in BRAFV600E Mutant Anaplastic Thyroid Cancer: A Single-Center Retrospective Cohort Study
- PMID: 36762947
- PMCID: PMC10122263
- DOI: 10.1089/thy.2022.0504
Surgery After BRAF-Directed Therapy Is Associated with Improved Survival in BRAFV600E Mutant Anaplastic Thyroid Cancer: A Single-Center Retrospective Cohort Study
Abstract
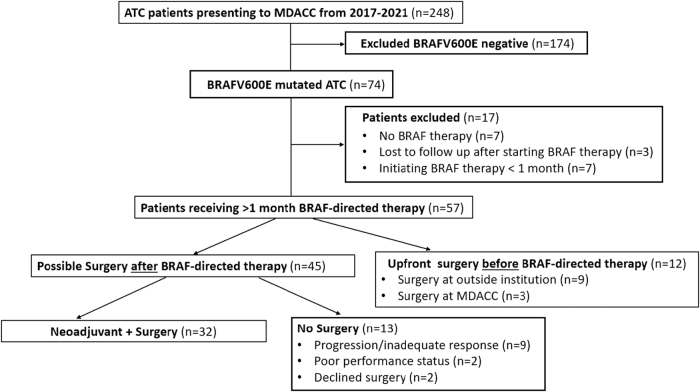
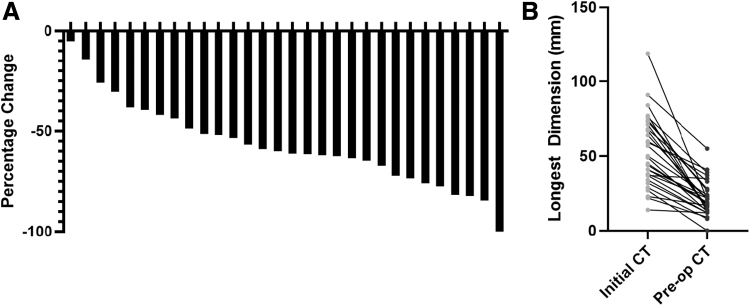
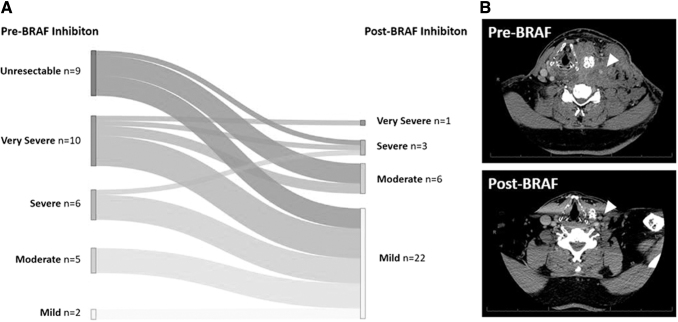
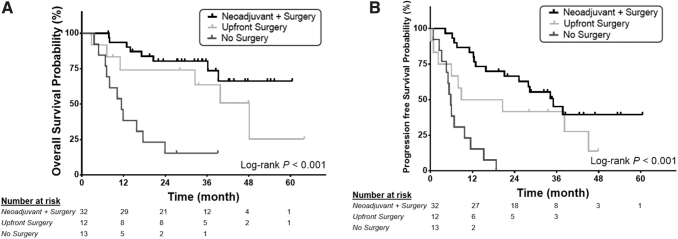
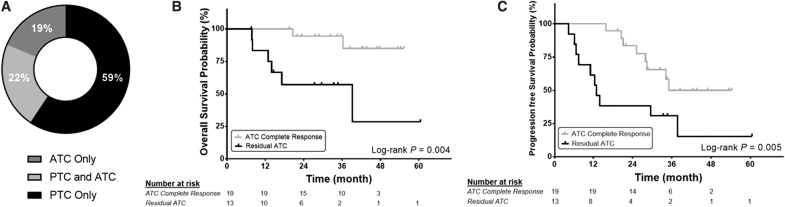
Background: The aim of this study was to describe the oncologic outcomes of patients with BRAFV600E-mutated anaplastic thyroid cancer (ATC) who had neoadjuvant BRAF-directed therapy with subsequent surgery. For context, we also reviewed patients who received BRAF-directed therapy after surgery, and those who did not have surgery after BRAF-directed therapy. Methods: This was a single-center retrospective cohort study conducted at a tertiary care cancer center in Texas from 2017 to 2021. Fifty-seven consecutive patients with BRAFV600E-mutated ATC and at least 1 month of BRAF-directed therapy were included. Primary outcomes were overall survival (OS) and progression-free survival (PFS). Results: All patients had stage IVB (35%) or IVC (65%) ATC. Approximately 70% of patients treated with BRAF-directed therapy ultimately had surgical resection of residual disease. Patients who had neoadjuvant BRAF-directed therapy followed by surgery (n = 32) had 12-month OS of 93.6% [confidence interval (CI) 84.9-100] and PFS of 84.4% [CI 71.8-96.7]. Patients who had surgery before BRAF-directed therapy (n = 12) had 12-month OS of 74.1% [CI 48.7-99.5] and PFS of 50% [CI 21.7-78.3]. Finally, patients who did not receive surgery after BRAF-directed therapy (n = 13) had 12-month OS of 38.5% [CI 12.1-64.9] and PFS of 15.4% [CI 0-35.0]. Neoadjuvant BRAF-directed therapy reduced tumor size, extent of surgery, and surgical morbidity score. Subgroup analysis suggested that any residual ATC in the surgical specimen was associated with significantly worse 12-month OS and PFS (OS = 83.3% [CI 62.6-100], PFS = 61.5% [CI 35.1-88]) compared with patients with pathologic ATC complete response (OS = 100%, PFS = 100%). Conclusions: We observed that neoadjuvant BRAF-directed therapy reduced extent of surgery and surgical morbidity. While acknowledging potential selection bias, the 12-month OS rate appeared higher in patients who had BRAF-directed therapy followed by surgery as compared with BRAF-directed therapy without surgery; yet, it was not significantly different from surgery followed by BRAF-directed therapy. PFS appeared higher in patients treated with neoadjuvant BRAF-directed therapy relative to patients in the other groups. These promising results of neoadjuvant BRAF-directed therapy followed by surgery for BRAF-mutated ATC should be confirmed in prospective clinical trials.
Keywords: BRAF therapy; BRAFV600E; anaplastic thyroid cancer; neoadjuvant; surgery; thyroid cancer.
Conflict of interest statement
M.D.W. is a member of the Bayer Scientific Advisory Board. M.E.C. has received grant funding from Genentech and Merk and has received consulting fees from Exelixis and Bayer. M.E.Z. has clinical research funding grants to MD Anderson Cancer Center from Merck and Eli Lilly. M.E.Z. is an Associate Editor at Thyroid but he had no role in the review of this manuscript and was blinded to the peer review processes.
Figures
Comment in
-
Anaplastic Thyroid Cancer: Shifting Paradigms-A Ray of Hope.Thyroid. 2023 Apr;33(4):402-403. doi: 10.1089/thy.2023.29150.sha. Epub 2023 Feb 28. Thyroid. 2023. PMID: 36856459 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
