

The impact of preoperative kidney replacement therapy on kidney outcome and survival in patients with left ventricular assist device
- PMID: 36763000
- PMCID: PMC9930763
- DOI: 10.1080/0886022X.2022.2157285
The impact of preoperative kidney replacement therapy on kidney outcome and survival in patients with left ventricular assist device
Abstract
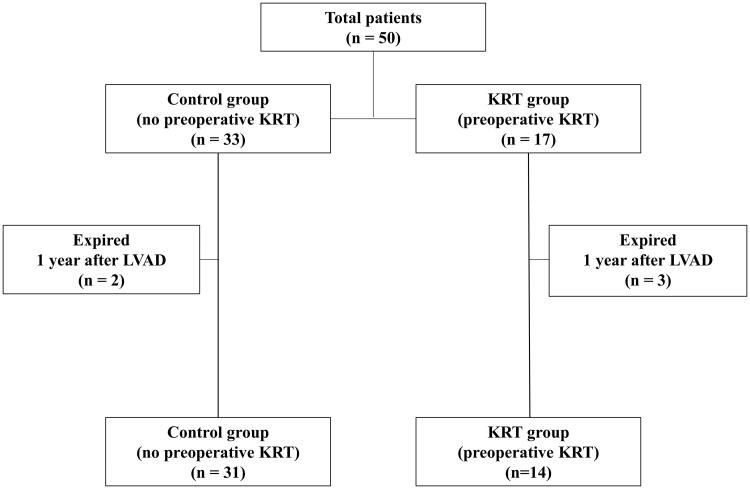
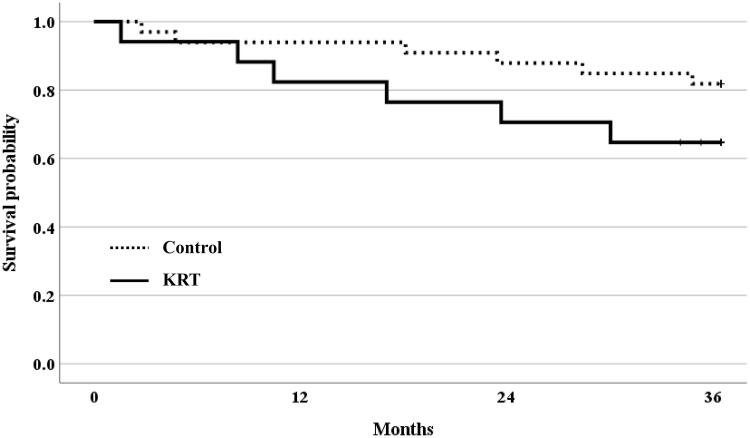
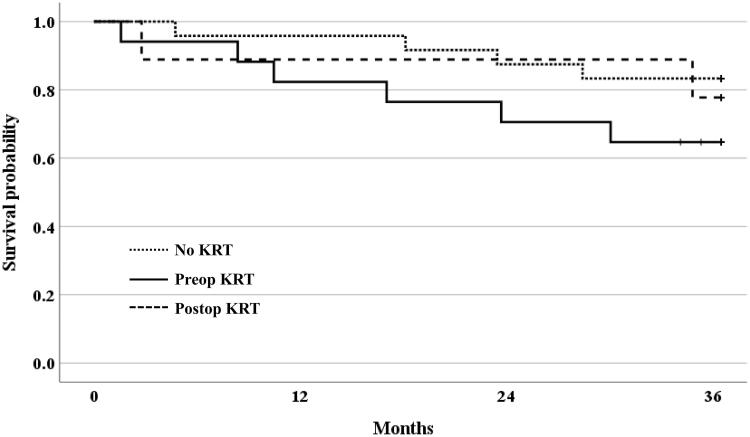
Left ventricular assist device (LVAD) has been highlighted as a new treatment option in the end-stage heart failure (HF). Kidney outcome after LVAD in severe cardiorenal syndrome (CRS) patients requiring kidney replacement therapy (KRT) is unclear. We investigated the impact of preoperative KRT on kidney function and survival in LVAD patients with severe CRS. A total of 50 patients followed up for at least 1 year after LVAD implantation was analyzed. The primary outcomes were estimated glomerular filtration rate and survival rate. Patients were divided into two groups depending on in-hospital KRT before LVAD implantation: the control group (n = 33) and the KRT group (n = 17). Postoperative KRT was performed for 76.5% of patients in the KRT group, and all of them discontinued KRT before discharge. There were no statistically significant differences in the degree of eGFR decline in survivors according to preoperative KRT. Although there were no statistically significant differences in the degree of eGFR decline in survivors regardless of preoperative KRT, old age (β -0.94, p < 0.01), preexisting chronic kidney disease (β -21.89, p < 0.01), and high serum creatinine (β -13.95, p < 0.01) were identified as independent predictors of post-LVAD eGFR decline. Mortality rate was higher, and more patients progressed to end-stage kidney disease in KRT group than control group. However, LVAD still can be considered as the treatment option in end-stage HF patients with severe CRS requiring KRT, especially in those with young age and previous normal kidney function.
Keywords: Cardiorenal syndrome; heart failure; kidney function; left ventricular assist device.
Conflict of interest statement
No potential conflict of interest was reported by the author(s).
Figures


Similar articles
-
Recovery after acute kidney injury requiring kidney replacement therapy in patients with left ventricular assist device: A meta-analysis.World J Crit Care Med. 2021 Nov 9;10(6):390-400. doi: 10.5492/wjccm.v10.i6.390. eCollection 2021 Nov 9. World J Crit Care Med. 2021. PMID: 34888164 Free PMC article.
-
Heart, kidney and left ventricular assist device: a complex trio.Eur J Clin Invest. 2021 Dec;51(12):e13662. doi: 10.1111/eci.13662. Epub 2021 Aug 17. Eur J Clin Invest. 2021. PMID: 34347897 Review.
-
Left Ventricular Assist Devices and the Kidney.Clin J Am Soc Nephrol. 2018 Feb 7;13(2):348-355. doi: 10.2215/CJN.04670417. Epub 2017 Oct 25. Clin J Am Soc Nephrol. 2018. PMID: 29070522 Free PMC article. Review.
-
Predictors of renal replacement therapy in patients with continuous flow left ventricular assist devices.J Artif Organs. 2021 Jun;24(2):207-216. doi: 10.1007/s10047-020-01239-z. Epub 2021 Feb 18. J Artif Organs. 2021. PMID: 33598826
-
Cystatin C- Versus Creatinine-Based Assessment of Renal Function and Prediction of Early Outcomes Among Patients With a Left Ventricular Assist Device.Circ Heart Fail. 2020 Jan;13(1):e006326. doi: 10.1161/CIRCHEARTFAILURE.119.006326. Epub 2020 Jan 21. Circ Heart Fail. 2020. PMID: 31959016
References
-
- Lund LH, Khush KK, Cherikh WS, et al. . The Registry of the International Society for Heart and Lung Transplantation: Thirty-fourth Adult Heart Transplantation Report-2017; focus theme: allograft ischemic time. J Heart Lung Transplant. 2017;36(10):1037–1046. - PubMed
-
- Benjamin EJ, Muntner P, Alonso A, et al. . Heart disease and stroke statistics-2019 update: a report from the American Heart Association. Circulation. 2019;139(10):e56–e528. - PubMed
-
- Rogers JG, Pagani FD, Tatooles AJ, et al. . Intrapericardial left ventricular assist device for advanced heart failure. N Engl J Med. 2017;376(5):451–460. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous