

Perioperative chemotherapy with 5-FU, leucovorin, oxaliplatin, and docetaxel (FLOT) for esophagogastric adenocarcinoma: ten years real-life experience from a surgical perspective
- PMID: 36763220
- PMCID: PMC9918580
- DOI: 10.1007/s00423-023-02822-7
Perioperative chemotherapy with 5-FU, leucovorin, oxaliplatin, and docetaxel (FLOT) for esophagogastric adenocarcinoma: ten years real-life experience from a surgical perspective
Abstract
Purpose: According to the results of FLOT4 trial, perioperative FLOT chemotherapy improved overall survival (OS) in locally advanced, resectable esophagogastric adenocarcinoma (EGA) compared to perioperative ECF/ECX. We report real-life data 10 years after introduction of perioperative FLOT at our institution.
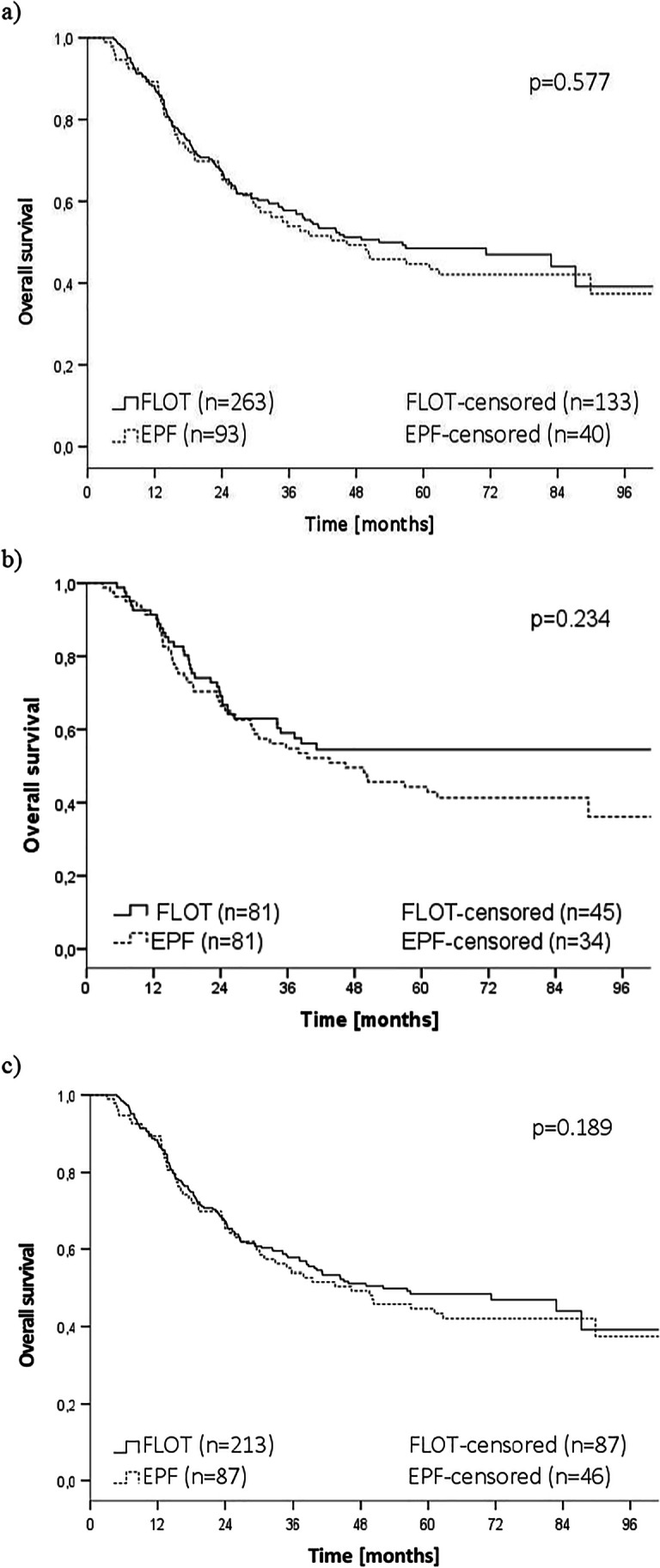
Methods: Survival of 356 consecutive EGA patients (cT3/4 and/or cN + and/or cM1) who underwent curative surgical resection was retrospectively analysed from a prospective database. A total of 263 patients received preoperative chemotherapy according to FLOT protocol and 93 patients received an epirubicin/platinum/5FU-based regimen (EPF). Propensity score matching (PSM) according to pretretment characteristics was performed to compensate for heterogeneity between groups.
Results: Median OS did not differ between groups (FLOT/EPF 52.1/46.4 months, p = 0.577). After PSM, survival was non-significantly improved after FLOT compared to EPF (median OS not reached/46.4 months, p = 0.156). Perioperative morbidity and mortality did not differ between groups. Histopathologic response rate was 35% after FLOT and 26% after EPF (p = 0.169). R0 resection could be achieved more frequently after FLOT than after EPF (93%/79%, p = 0.023).
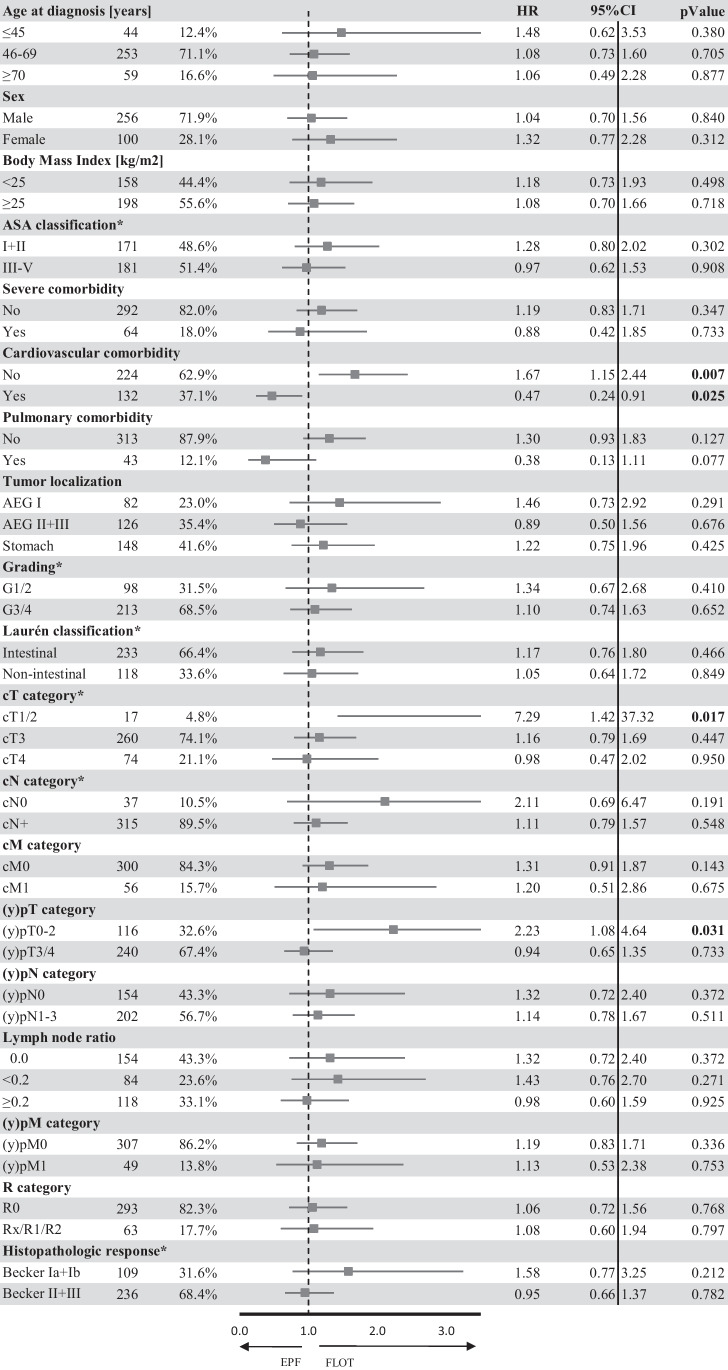
Conclusion: Overall survival after perioperative FLOT followed by surgery is comparable to clinical trials. However, collective real-life application of FLOT failed to provide a significant survival benefit compared to EPF. In clinical reality, patient selection is triggered by age, comorbidity, tumor localization, and clinical tumor stage. Yet matched analyses support FLOT4 trial findings.
Keywords: Adenocarcinoma; Esophageal cancer; Gastric cancer; Histopathological regression; Perioperative chemotherapy.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
The authors declare that they do not have any commercial interest in the subject of study.
The authors did not receive financial support or funding for conduction of this study.
GM Haag reports fees for advisory role from Sanofi, Roche, Taiho, Nordic, Lilly, Pfizer, honoraria from Roche, travel grants from Amgen, Ipsen and Celgene; research funding is provided by Nordic and Taiho Pharmaceuticals. There is no relationship to the submitted work.
Figures

Similar articles
-
Histopathological regression after neoadjuvant docetaxel, oxaliplatin, fluorouracil, and leucovorin versus epirubicin, cisplatin, and fluorouracil or capecitabine in patients with resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4-AIO): results from the phase 2 part of a multicentre, open-label, randomised phase 2/3 trial.Lancet Oncol. 2016 Dec;17(12):1697-1708. doi: 10.1016/S1470-2045(16)30531-9. Epub 2016 Oct 22. Lancet Oncol. 2016. PMID: 27776843 Clinical Trial.
-
Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): a randomised, phase 2/3 trial.Lancet. 2019 May 11;393(10184):1948-1957. doi: 10.1016/S0140-6736(18)32557-1. Epub 2019 Apr 11. Lancet. 2019. PMID: 30982686 Clinical Trial.
-
Implementation of perioperative FLOT compared to ECX/EOX chemotherapy regimens in resectable esophagogastric adenocarcinomas: an analysis of real-world data.Acta Oncol. 2024 May 14;63:322-329. doi: 10.2340/1651-226X.2024.35431. Acta Oncol. 2024. PMID: 38745482 Free PMC article.
-
[Does the FLOT regimen a new standard of perioperative chemotherapy for localized gastric cancer?].Bull Cancer. 2020 Jan;107(1):54-60. doi: 10.1016/j.bulcan.2019.12.005. Epub 2020 Jan 21. Bull Cancer. 2020. PMID: 31980145 Review. French.
-
FLOT or CROSS for gastroesophageal junction cancers-is the debate over yet?Chin Clin Oncol. 2023 Jun;12(3):24. doi: 10.21037/cco-23-5. Epub 2023 May 25. Chin Clin Oncol. 2023. PMID: 37303220 Review.
Cited by
-
Clinical Characteristics and Oncological Outcomes of Surgically Treated Early-Onset Gastric Adenocarcinoma - a Retrospective Cohort Study.J Cancer. 2023 May 21;14(9):1470-1478. doi: 10.7150/jca.82876. eCollection 2023. J Cancer. 2023. PMID: 37325055 Free PMC article.
-
ASO Author Reflections: The Role of Beta-Blockers in Gastric Cancer-A Pathway to Personalized Therapy?Ann Surg Oncol. 2025 Jul;32(7):5202-5203. doi: 10.1245/s10434-025-17326-5. Epub 2025 Apr 24. Ann Surg Oncol. 2025. PMID: 40272666 Free PMC article. No abstract available.
-
Targeted therapies in neoadjuvant treatment for gastroesophageal cancer.Ecancermedicalscience. 2025 Jun 3;19:1921. doi: 10.3332/ecancer.2025.1921. eCollection 2025. Ecancermedicalscience. 2025. PMID: 40606954 Free PMC article. Review.
-
Outcomes of locally advanced gastric and gastroesophageal adenocarcinoma cancers treated with neoadjuvant FLOT in a tertiary care hospital in Pakistan.Ecancermedicalscience. 2024 May 21;18:1705. doi: 10.3332/ecancer.2024.1705. eCollection 2024. Ecancermedicalscience. 2024. PMID: 39021541 Free PMC article.
-
Perioperative Chemotherapy for Gastro-Esophageal or Gastric Cancer: Anthracyclin Triplets versus FLOT.Cancers (Basel). 2024 Mar 26;16(7):1291. doi: 10.3390/cancers16071291. Cancers (Basel). 2024. PMID: 38610969 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
