

The Use and Effectiveness of Ceftazidime-Avibactam in Real-World Clinical Practice: EZTEAM Study
- PMID: 36763243
- PMCID: PMC9912999
- DOI: 10.1007/s40121-023-00762-9
The Use and Effectiveness of Ceftazidime-Avibactam in Real-World Clinical Practice: EZTEAM Study
Abstract
Introduction: Ceftazidime-avibactam has proven activity against multidrug-resistant (MDR) bacteria in clinical trials and real-world studies. This study was conducted to describe the patterns of use of ceftazidime-avibactam (including indications and associated antibiotics), and the effectiveness and safety of ceftazidime-avibactam in real-world clinical practice.
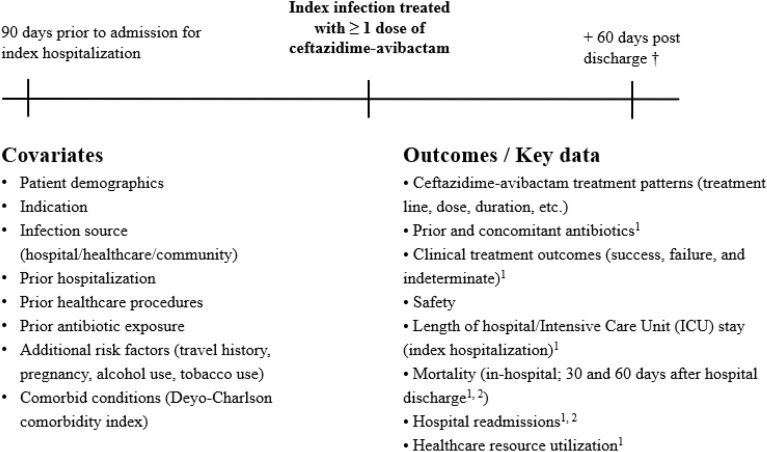
Methods: This non-interventional medical chart review study was conducted in 11 countries across the European and Latin American (LATAM) regions. Consecutive patients treated in clinical practice with at least one dose of ceftazidime-avibactam for an approved indication per country label since 01 January 2018 (or launch date in the country if posterior) were enrolled. Effectiveness analyses were conducted in patients treated with ceftazidime-avibactam for at least 72 h.
Results: Of the 569 eligible patients enrolled, 516 (90.7%) were treated for at least 72 h (354 patients from Europe and 162 patients from LATAM); 390 patients (75.7%) had switched from another antibiotic line for Gram-negative coverage. Infection sources were intra-abdominal, urinary, respiratory, bloodstream infections, and other infections (approximately 20% each). K. pneumoniae was the most common microorganism identified in the latest microbiological evaluation before starting ceftazidime-avibactam (59.3%). Two-thirds of microorganisms tested for susceptibility were MDR, of which 89.3% were carbapenem-resistant. The common MDR mechanisms for K. pneumoniae were carbapenemase (33.9%), oxacillinase 48 (25.2%), extended-spectrum beta-lactamase (21.5%), or metallo-beta-lactamase (14.2%) production. Without prior patient exposure, 17 isolates (mostly K. pneumoniae) were resistant to ceftazidime-avibactam. Treatment success was achieved in 77.3% of patients overall (88.3% among patients with urinary infection), regardless of first or second treatment line. In-hospital mortality rate was 23.1%. Adverse events were reported for six of the 569 patients enrolled.
Conclusion: This study provides important real-world evidence on treatment patterns, effectiveness, and safety of ceftazidime-avibactam in clinical practice through its recruitment in the European and LATAM regions. Ceftazidime-avibactam is one of the antibiotics to consider for treatment of MDR bacteria.
Trial registration: ClinicalTrials.gov identifier, NCT03923426.
Keywords: Bloodstream infection; Ceftazidime–avibactam; Europe; Intra-abdominal infection; K. pneumoniae; LATAM; Multidrug-resistant; Respiratory infection; Urinary infection.
© 2023. The Author(s).
Figures
References
-
- Zarb P, Coignard B, Griskeviciene J, et al. The European Centre for Disease Prevention and Control (ECDC) pilot point prevalence survey of healthcare-associated infections and antimicrobial use. Euro Surveill. 2012. 10.2807/ese.17.46.20316-en. - PubMed
-
- World Health Organizations. Annual epidemiological report on communicable disease in Europe. 2008. https://ecdc.europa.eu/sites/portal/files/media/en/publications/Publicat.... Accessed 22 Feb 2018.
-
- Annual epidemiological report Reporting on 2011 surveillance data and 2012 epidemic intelligence data. 2013. https://www.ecdc.europa.eu/sites/default/files/media/en/publications/Pub.... Accessed 21 Oct 2021.
Associated data
LinkOut - more resources
Full Text Sources
Medical
