

Association of Modifiable Health Conditions and Social Determinants of Health With Late Mortality in Survivors of Childhood Cancer
- PMID: 36763361
- PMCID: PMC9918884
- DOI: 10.1001/jamanetworkopen.2022.55395
Association of Modifiable Health Conditions and Social Determinants of Health With Late Mortality in Survivors of Childhood Cancer
Abstract
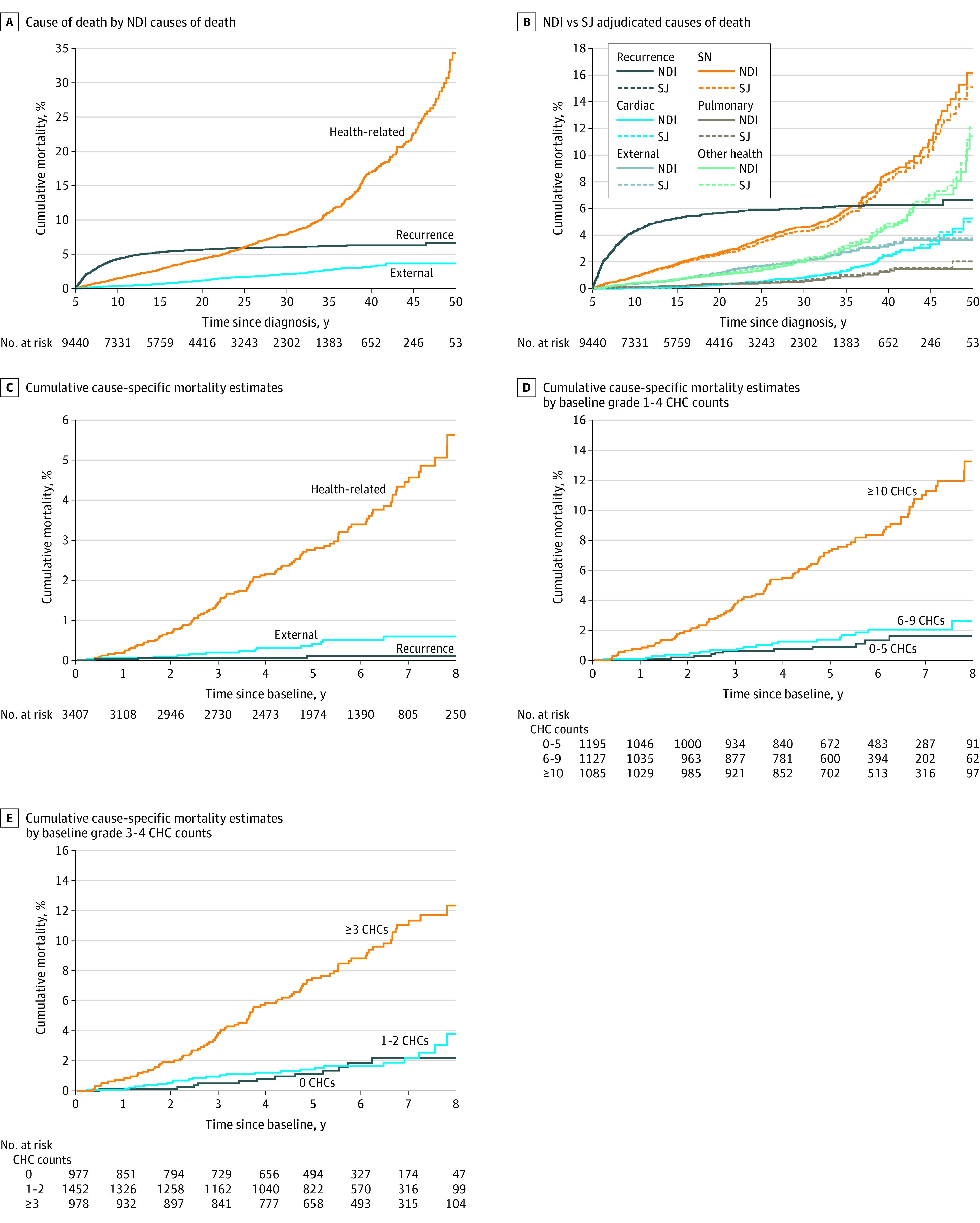
Importance: Associations between modifiable chronic health conditions (CHCs), social determinants of health, and late mortality (defined as death occurring ≥5 years after diagnosis) in childhood cancer survivors are unknown.
Objective: To explore associations between modifiable CHCs and late mortality within the context of social determinants of health.
Design, setting, and participants: This longitudinal cohort study used data from 9440 individuals who were eligible to participate in the St Jude Lifetime Cohort (SJLIFE), a retrospective cohort study with prospective clinical follow-up that was initiated in 2007 to characterize outcomes among childhood cancer survivors. Eligible individuals had survived 5 or more years after childhood cancer diagnosis, were diagnosed between 1962 and 2012, and received treatment at St Jude Children's Research Hospital were included in mortality estimates. A total of 3407 adult SJLIFE participants (aged ≥18 years) who completed an on-campus assessment were included in risk factor analyses. Vital status, date of death, and cause of death were obtained by linkage with the National Death Index (coverage from inception to December 31, 2016). Deaths occurring before inception of the National Death Index were obtained from the St Jude Children's Research Hospital Cancer Registry. Data were analyzed from June to December 2022.
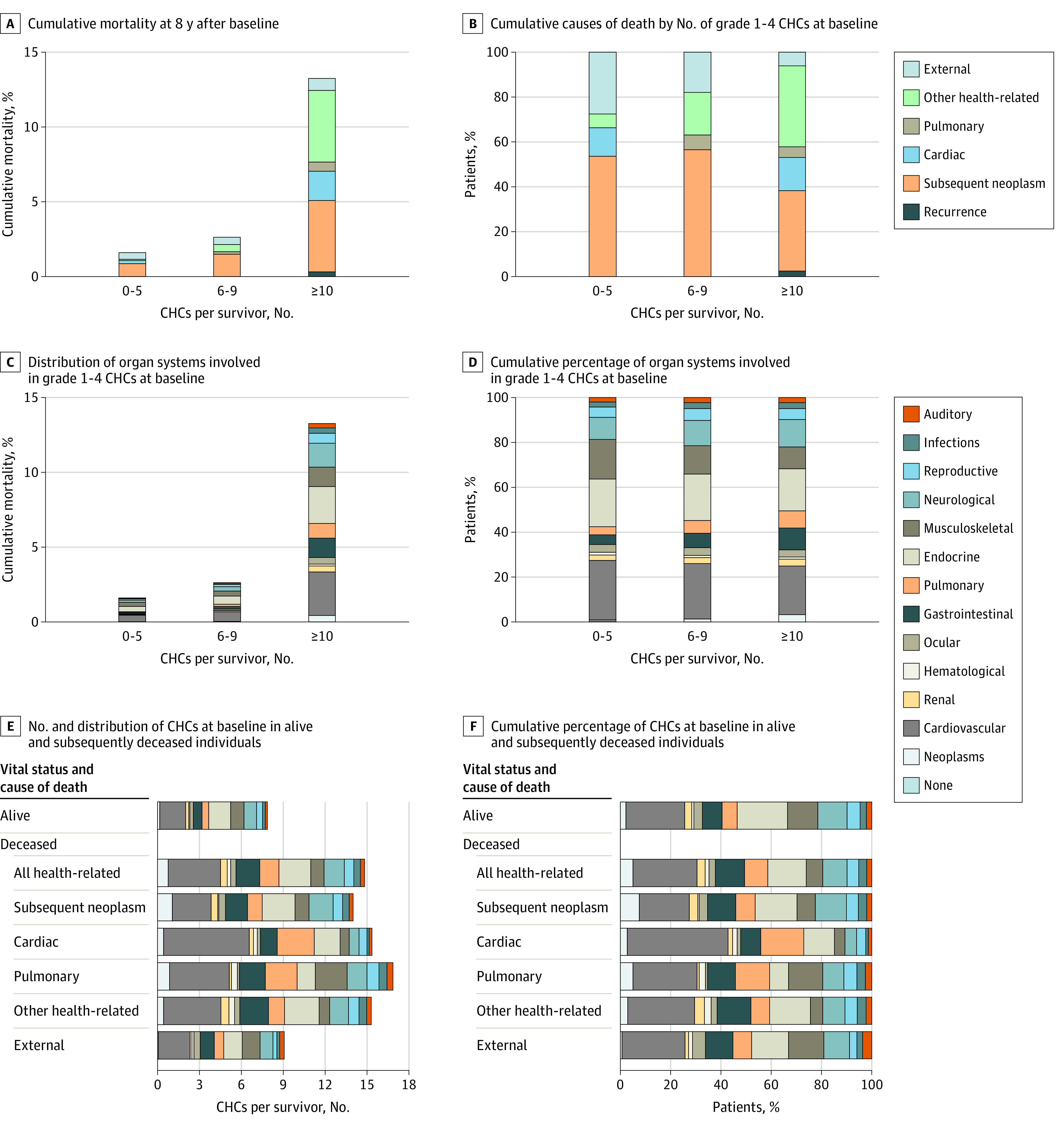
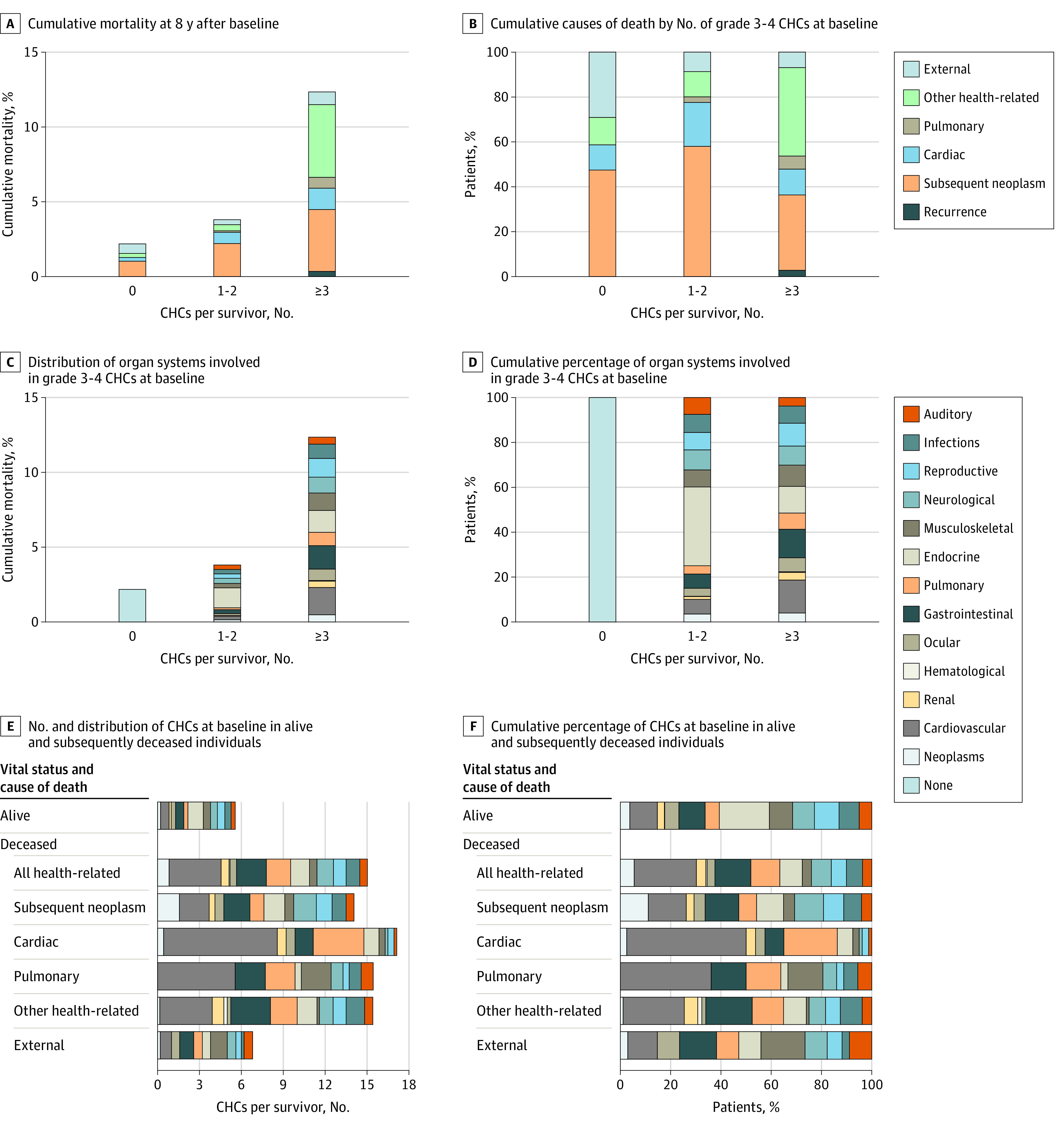
Exposures: Data on treatment exposures and causes of death were abstracted for individuals who were eligible to participate in the SJLIFE study. Information on modifiable CHCs (dyslipidemia, hypertension, diabetes, underweight or obesity, bone mineral deficiency, hypogonadism, hypothyroidism, and adrenal insufficiency, all graded by the modified Common Terminology Criteria for Adverse Events), healthy lifestyle index (smoking status, alcohol consumption, body mass index [calculated as weight in kilograms divided by height in meters squared], and physical activity), area deprivation index (ADI; which measures neighborhood-level socioeconomic disadvantage), and frailty (low lean muscle mass, exhaustion, low energy expenditure, slowness, and weakness) was obtained for participants.
Main outcomes and measures: National Death Index causes of death were used to estimate late mortality using standardized mortality ratios (SMRs) and 95% CIs, which were calculated based on US mortality rates. For the risk factor analyses (among participants who completed on-campus assessment), multivariable piecewise exponential regression analysis was used to estimate rate ratios (RRs) and 95% CIs for all-cause and cause-specific late mortality.
Results: Among 9440 childhood cancer survivors who were eligible to participate in the SJLIFE study, the median (range) age at assessment was 27.5 (5.3-71.9) years, and the median (range) duration of follow-up was 18.8 (5.0-58.0) years; 55.2% were male and 75.3% were non-Hispanic White. Survivors experienced increases in all-cause mortality (SMR, 7.6; 95% CI, 7.2-8.1) and health-related late mortality (SMR, 7.6; 95% CI, 7.0-8.2). Among 3407 adult SJLIFE participants who completed an on-campus assessment, the median (range) age at assessment was 35.4 (17.9-69.8) years, and the median (range) duration of follow-up was 27.3 (7.3-54.7) years; 52.5% were male and 81.7% were non-Hispanic White. Models adjusted for attained age, sex, race and ethnicity, age at diagnosis, treatment exposures, household income, employment status, and insurance status revealed that having 1 modifiable CHC of grade 2 or higher (RR, 2.2; 95% CI, 1.2-4.0; P = .01), 2 modifiable CHCs of grade 2 or higher (RR, 2.6; 95% CI, 1.4-4.9; P = .003), or 3 modifiable CHCs of grade 2 or higher (RR, 3.6; 95% CI, 1.8-7.1, P < .001); living in a US Census block with an ADI in the 51st to 80th percentile (RR, 5.5; 95% CI, 1.3-23.5; P = .02), an ADI in the 81st to 100th percentile (RR, 8.7; 95% CI, 2.0-37.6; P = .004), or an unassigned ADI (RR, 15.7; 95% CI, 3.5-70.3; P < .001); and having frailty (RR, 2.3; 95% CI, 1.3-3.9; P = .004) were associated with significant increases in the risk of late all-cause death. Similar associations were observed for the risk of late health-related death (1 modifiable CHC of grade ≥2: RR, 2.2 [95% CI, 1.1-4.4; P = .02]; 2 modifiable CHCs of grade ≥2: RR, 2.5 [95% CI, 1.2-5.2; P = .01]; 3 modifiable CHCs of grade ≥2: RR, 4.0 [95% CI, 1.9-8.4; P < .001]; ADI in 51st-80th percentile: RR, 9.2 [95% CI, 1.2-69.7; P = .03]; ADI in 81st-100th percentile: RR, 16.2 [95% CI, 2.1-123.7; P = .007], unassigned ADI: RR, 27.3 [95% CI, 3.5-213.6; P = .002]; and frailty: RR, 2.3 [95% CI, 1.2-4.1; P = .009]).
Conclusions and relevance: In this cohort study of childhood cancer survivors, living in a Census block with a high ADI and having modifiable CHCs were independently associated with an increased risk of late death among survivors of childhood cancer. Future investigations seeking to mitigate these factors will be important to improving health outcomes and developing risk-stratification strategies to optimize care delivery to childhood cancer survivors.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
