

Resection of NAFLD/NASH-related Hepatocellular Carcinoma (HCC): Clinical Features and Outcomes Compared with HCC Due to Other Etiologies
- PMID: 36763374
- PMCID: PMC10078904
- DOI: 10.1093/oncolo/oyac251
Resection of NAFLD/NASH-related Hepatocellular Carcinoma (HCC): Clinical Features and Outcomes Compared with HCC Due to Other Etiologies
Abstract
Background: Non-alcoholic fatty liver disease (NAFLD) and non-alcoholic steatohepatitis (NASH) are the leading causes of hepatocellular carcinoma (HCC) worldwide. Limited data exist on surgical outcomes for NAFLD/NASH-related HCC compared with other HCC etiologies. We evaluated differences in clinicopathological characteristics and outcomes of patients undergoing surgical resection for NAFLD/NASH-associated HCC compared with other HCC etiologies.
Methods: Demographic, clinicopathological features, and survival outcomes of patients with surgically resected HCC were collected. NAFLD activity score (NAS) and fibrosis score were assessed by focused pathologic review in a subset of patients.
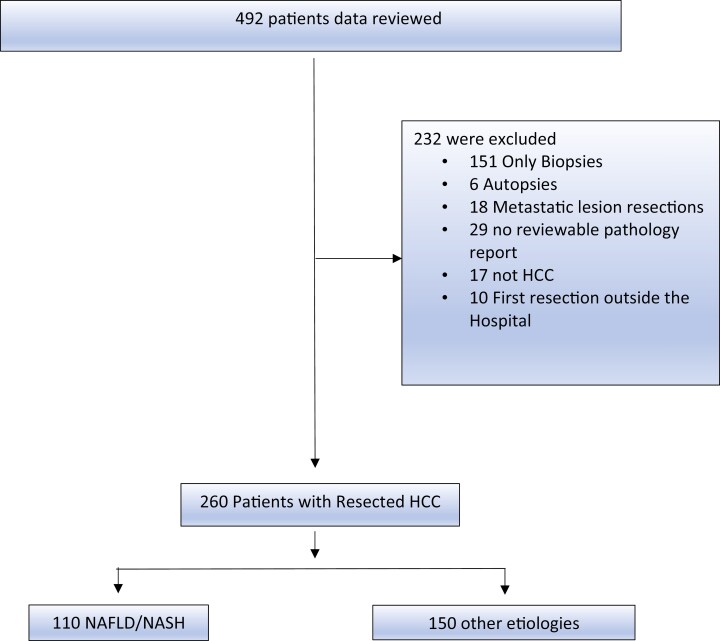
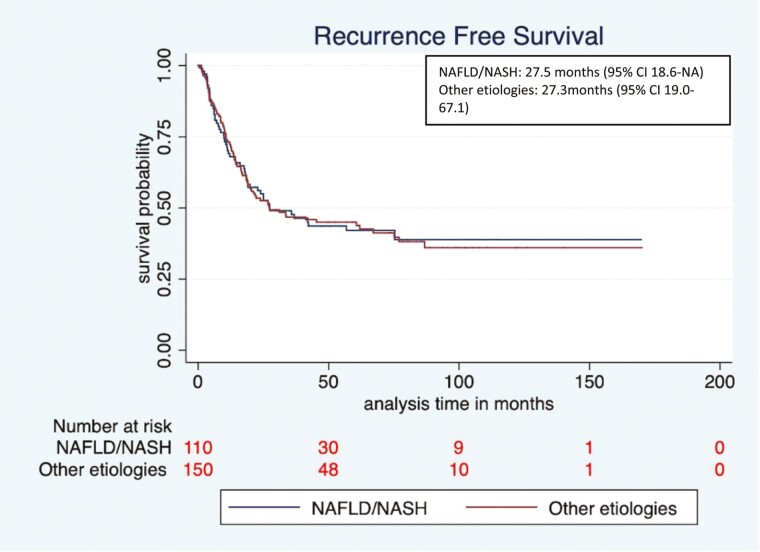
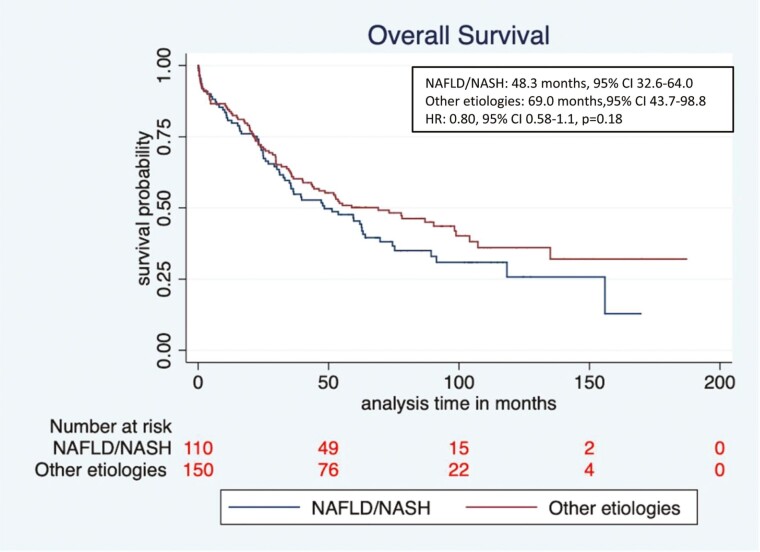
Results: Among 492 patients screened, 260 met eligibility (NAFLD/NASH [n = 110], and other etiologies [n = 150]). Median age at diagnosis was higher in the NAFLD/NASH HCC cohort compared with the other etiologies cohort (66.7 vs. 63.4 years, respectively, P = .005), with an increased percentage of female patients (36% vs. 18%, P = .001). NAFLD/NASH-related tumors were more commonly >5 cm (66.0% vs. 45%, P = .001). There were no significant differences in rates of lymphovascular or perineural invasion, histologic grade, or serum AFP levels. The NAFLD/NASH cohort had lower rates of background liver fibrosis, lower AST and ALT levels, and higher platelet counts (P < .01 for all). Median overall survival (OS) was numerically shorter in NAFLD/NASH vs other etiology groups, however, not statistically significant.
Conclusions: Patients with NAFLD/NASH-related HCC more commonly lacked liver fibrosis and presented with larger HCCs compared with patients with HCC from other etiologies. No differences were seen in rates of other high-risk features or survival. With the caveat of sample size and retrospective analysis, this supports a similar decision-making approach regarding surgical resection for NAFLD/NASH and other etiology-related HCCs.
Keywords: NAFLD; NASH; hepatocellular carcinoma; metabolic syndrome; outcome; steatohepatitis.
© The Author(s) 2023. Published by Oxford University Press.
Conflict of interest statement
Surendra Pal Chaudhary is a full-time employee at EMD Serono, Inc. Lipika Goyal reports receiving research funding (to institution) from Adaptimmune, Bayer, Eisai, Merck, Macrogenics, Genentech, Novartis, Incyte, Eli Lilly, Loxo Oncology, Relay Therapeutics, QED, Servier, Taiho Oncology, Leap Therapeutics, Bristol Meyers Squibb, and Nucana; she also serves as an advisor/consultant to Alentis Therapeutics, AstraZeneca, Exelixis, Genentech, H3Biomedicine, Kinnate, QED Therapeutics, Servier, Sirtex Medical Ltd., Taiho Oncology, Inc., and TranstheraBio. Jeffrey William Clark reports receiving research funding (to institution) from Eisai, Exelixis, Genentech, Surface Oncology, and Trisalus Life Sciences; he also receives consulting fees from Foundation Medicine. The other authors indicated no financial relationships.
Figures
References
-
- Puoti C. New insights on hepatocellular carcinoma: epidemiology and clinical aspects. Hepatoma Res. 2018;4:57. 10.20517/2394-5079.2018.67. - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
