

The human proton pump inhibitors inhibit Mycobacterium tuberculosis rifampicin efflux and macrophage-induced rifampicin tolerance
- PMID: 36763530
- PMCID: PMC7614234
- DOI: 10.1073/pnas.2215512120
The human proton pump inhibitors inhibit Mycobacterium tuberculosis rifampicin efflux and macrophage-induced rifampicin tolerance
Abstract
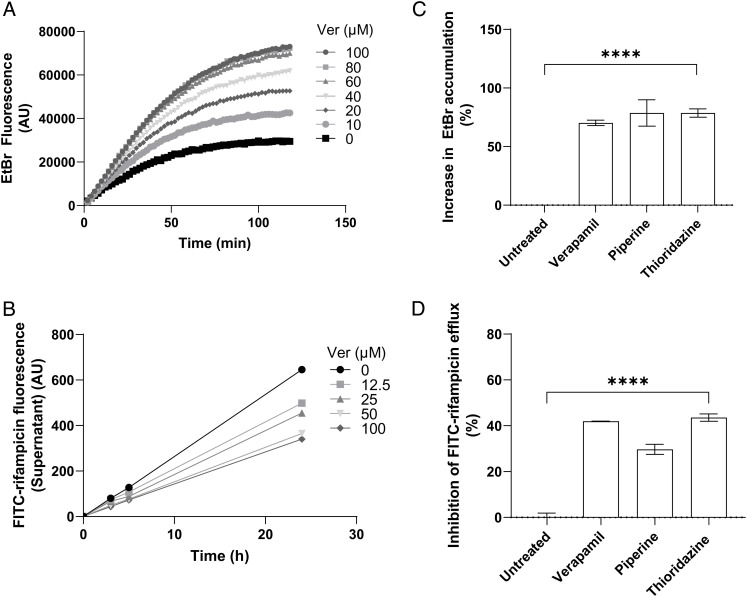
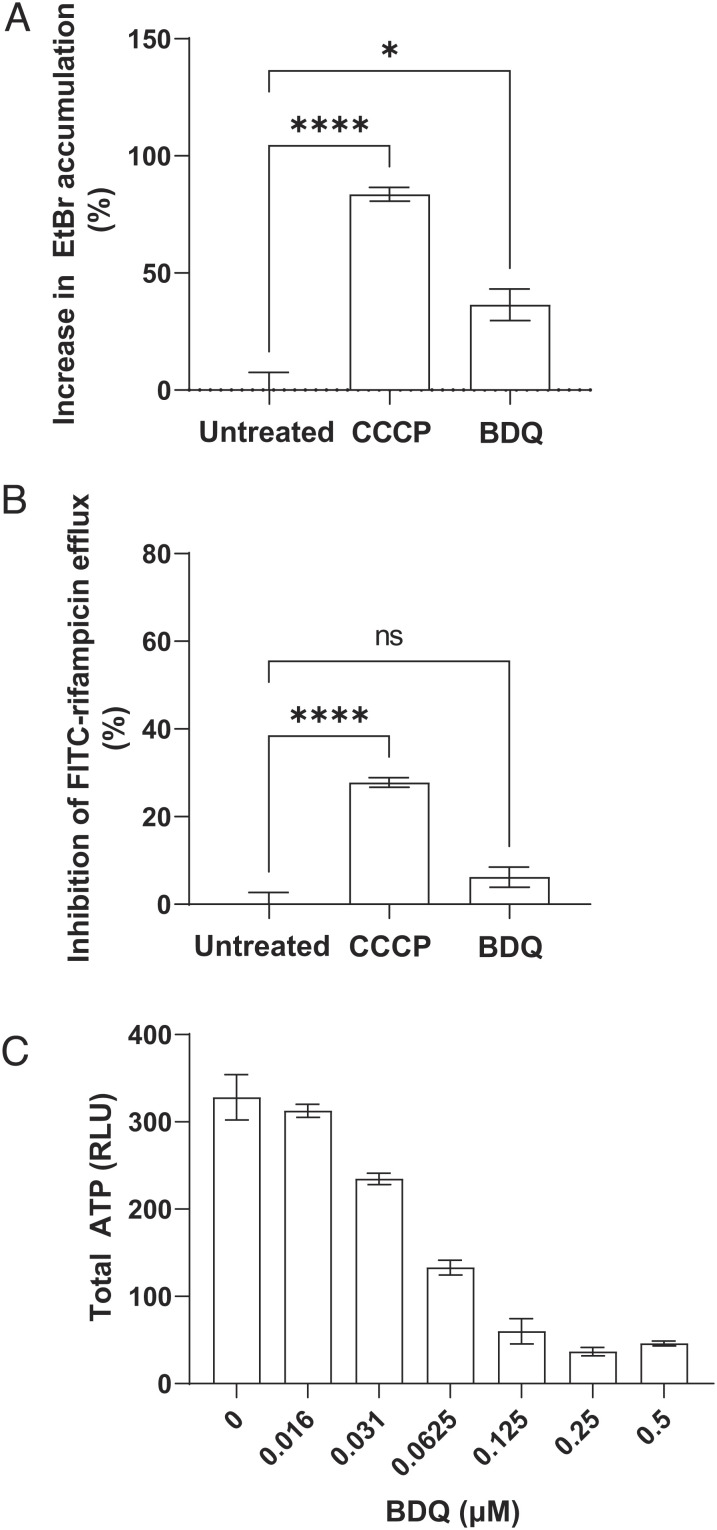
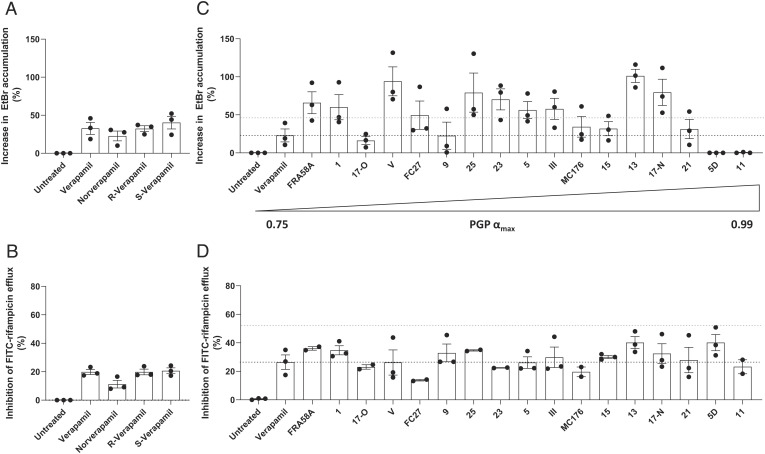
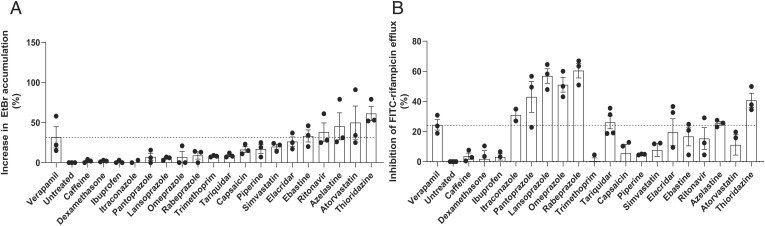
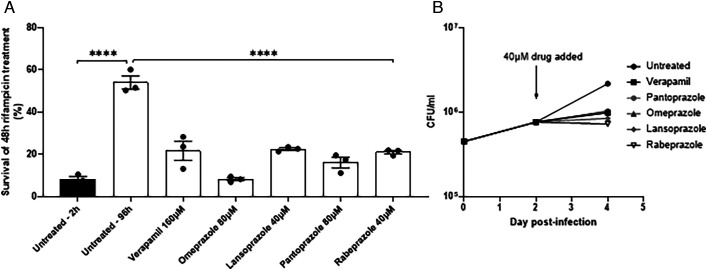
Tuberculosis treatment requires months-long combination chemotherapy with multiple drugs, with shorter treatments leading to relapses. A major impediment to shortening treatment is that Mycobacterium tuberculosis becomes tolerant to the administered drugs, starting early after infection and within days of infecting macrophages. Multiple lines of evidence suggest that macrophage-induced drug tolerance is mediated by mycobacterial drug efflux pumps. Here, using assays to directly measure drug efflux, we find that M. tuberculosis transports the first-line antitubercular drug rifampicin through a proton gradient-dependent mechanism. We show that verapamil, a known efflux pump inhibitor, which inhibits macrophage-induced rifampicin tolerance, also inhibits M.tuberculosis rifampicin efflux. As with macrophage-induced tolerance, the calcium channel-inhibiting property of verapamil is not required for its inhibition of rifampicin efflux. By testing verapamil analogs, we show that verapamil directly inhibits M. tuberculosis drug efflux pumps through its human P-glycoprotein (PGP)-like inhibitory activity. Screening commonly used drugs with incidental PGP inhibitory activity, we find many inhibit rifampicin efflux, including the proton pump inhibitors (PPIs) such as omeprazole. Like verapamil, the PPIs inhibit macrophage-induced rifampicin tolerance as well as intramacrophage growth, which has also been linked to mycobacterial efflux pump activity. Our assays provide a facile screening platform for M. tuberculosis efflux pump inhibitors that inhibit in vivo drug tolerance and growth.
Keywords: efflux pump inhibitors; mycobacterial efflux pumps; proton pump inhibitors; tuberculosis rifampicin tolerance; verapamil.
Conflict of interest statement
The authors declare no competing interest.
Figures
Similar articles
-
Xpert® MTB/RIF assay for extrapulmonary tuberculosis and rifampicin resistance.Cochrane Database Syst Rev. 2018 Aug 27;8(8):CD012768. doi: 10.1002/14651858.CD012768.pub2. Cochrane Database Syst Rev. 2018. Update in: Cochrane Database Syst Rev. 2021 Jan 15;1:CD012768. doi: 10.1002/14651858.CD012768.pub3. PMID: 30148542 Free PMC article. Updated.
-
Xpert MTB/XDR for detection of pulmonary tuberculosis and resistance to isoniazid, fluoroquinolones, ethionamide, and amikacin.Cochrane Database Syst Rev. 2022 May 18;5(5):CD014841. doi: 10.1002/14651858.CD014841.pub2. Cochrane Database Syst Rev. 2022. PMID: 35583175 Free PMC article.
-
Verapamil, and its metabolite norverapamil, inhibit macrophage-induced, bacterial efflux pump-mediated tolerance to multiple anti-tubercular drugs.J Infect Dis. 2014 Aug 1;210(3):456-66. doi: 10.1093/infdis/jiu095. Epub 2014 Feb 14. J Infect Dis. 2014. PMID: 24532601 Free PMC article.
-
Xpert® MTB/RIF assay for pulmonary tuberculosis and rifampicin resistance in adults.Cochrane Database Syst Rev. 2013 Jan 31;(1):CD009593. doi: 10.1002/14651858.CD009593.pub2. Cochrane Database Syst Rev. 2013. Update in: Cochrane Database Syst Rev. 2014 Jan 21;(1):CD009593. doi: 10.1002/14651858.CD009593.pub3. PMID: 23440842 Free PMC article. Updated.
-
Xpert MTB/RIF Ultra assay for tuberculosis disease and rifampicin resistance in children.Cochrane Database Syst Rev. 2022 Sep 6;9(9):CD013359. doi: 10.1002/14651858.CD013359.pub3. Cochrane Database Syst Rev. 2022. PMID: 36065889 Free PMC article.
Cited by
-
Redefining tuberculosis: an interview with Lalita Ramakrishnan.Dis Model Mech. 2023 Mar 1;16(3):dmm050189. doi: 10.1242/dmm.050189. Epub 2023 Mar 23. Dis Model Mech. 2023. PMID: 36951140 Free PMC article.
-
Profile of Lalita Ramakrishnan.Proc Natl Acad Sci U S A. 2023 Jun 13;120(24):e2306553120. doi: 10.1073/pnas.2306553120. Epub 2023 May 31. Proc Natl Acad Sci U S A. 2023. PMID: 37256924 Free PMC article. No abstract available.
-
A Dose-Finding Study to Guide Use of Verapamil as an Adjunctive Therapy in Tuberculosis.Clin Pharmacol Ther. 2024 Feb;115(2):324-332. doi: 10.1002/cpt.3108. Epub 2023 Dec 11. Clin Pharmacol Ther. 2024. PMID: 37983978 Free PMC article. Clinical Trial.
-
A virulence-associated small RNA MTS1338 activates an ABC transporter CydC for rifampicin efflux in Mycobacterium tuberculosis.Front Microbiol. 2024 Sep 19;15:1469280. doi: 10.3389/fmicb.2024.1469280. eCollection 2024. Front Microbiol. 2024. PMID: 39364170 Free PMC article.
-
Verapamil and its metabolite norverapamil inhibit the Mycobacterium tuberculosis MmpS5L5 efflux pump to increase bedaquiline activity.Proc Natl Acad Sci U S A. 2025 Apr 22;122(16):e2426827122. doi: 10.1073/pnas.2426827122. Epub 2025 Apr 17. Proc Natl Acad Sci U S A. 2025. PMID: 40244664 Free PMC article.
References
-
- East African/British Medical Research Councils, Controlled clinical trial of four short-course (6-month) regimens of chemotherapy for treatment of pulmonary tuberculosis. Second Report. Lancet 301, 1331–1339 (1973). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
