

Epileptic Status in a PEDiatric cohort (ESPED) requiring intensive care treatment: A multicenter, national, two-year prospective surveillance study
- PMID: 36764666
- PMCID: PMC10235585
- DOI: 10.1002/epi4.12707
Epileptic Status in a PEDiatric cohort (ESPED) requiring intensive care treatment: A multicenter, national, two-year prospective surveillance study
Abstract
Objective: The aim of this study was to provide seizure etiology, semiology, underlying conditions, and out-of- and in-hospital diagnostics, treatment, and outcome data on children with out-of- or in-hospital-onset status epilepticus (SE) according to the International League Against Epilepsy definition that required admission to the pediatric intensive care unit (PICU) for ≥4 hours.
Methods: This prospective national surveillance study on SE in childhood and adolescence was conducted over 2 years (07/2019-06/2021).
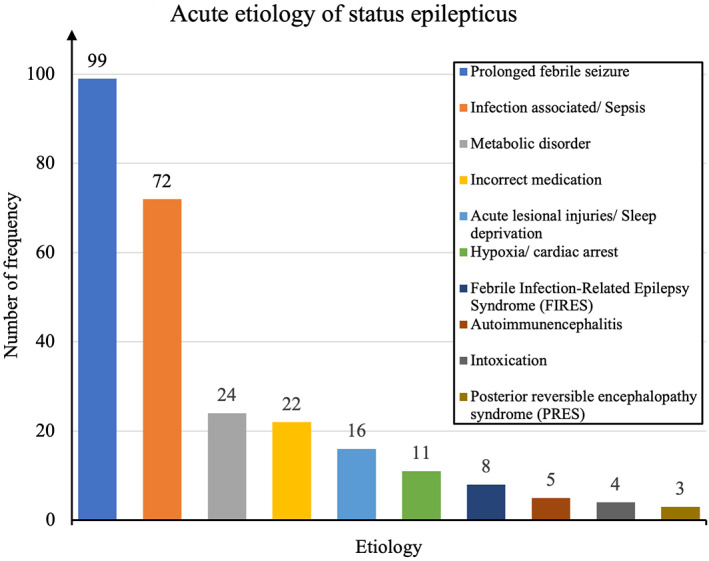
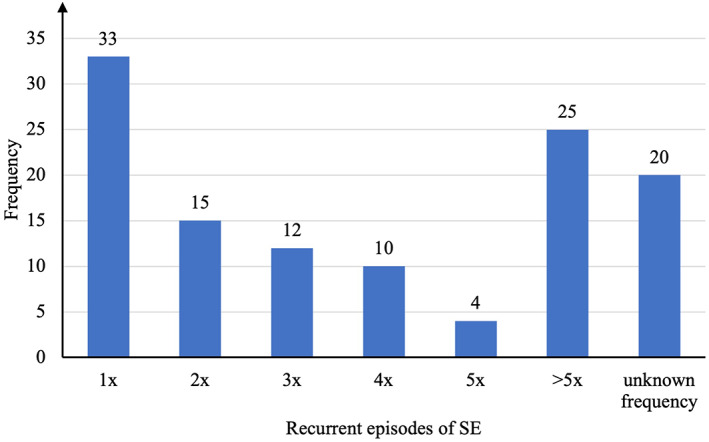
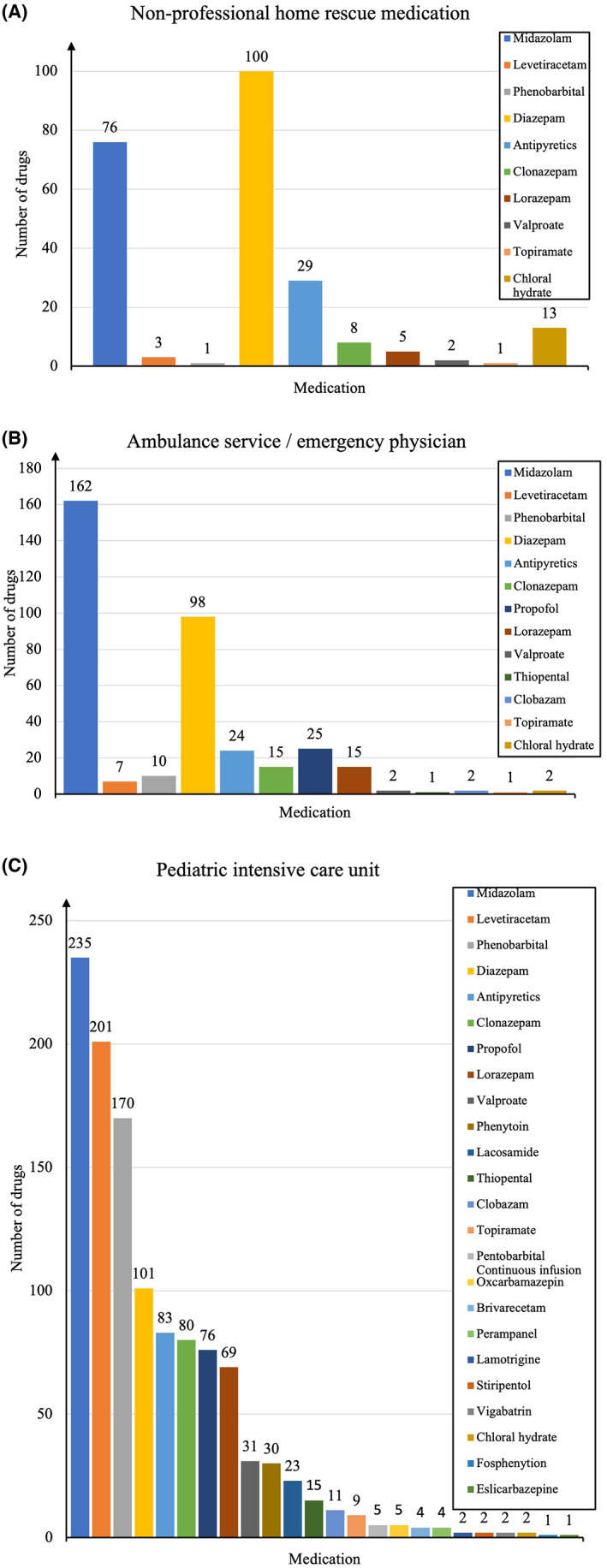
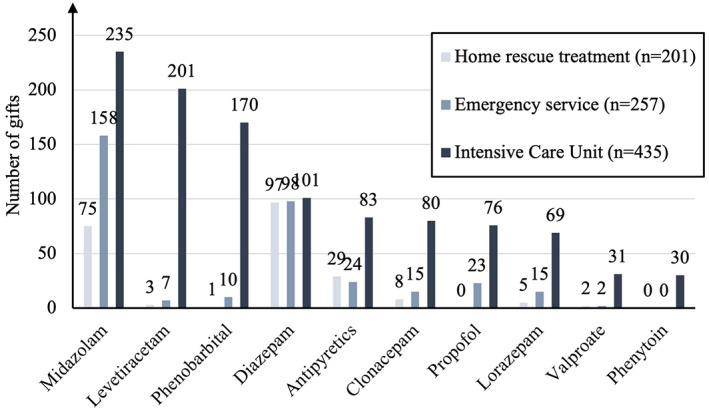
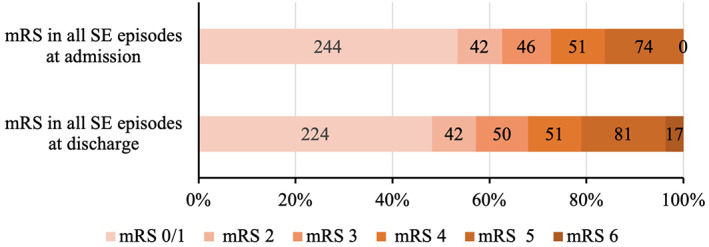
Results: This study examined 481 SE episodes in 481 children with a median age of 43 months (1 month to 17 years 11 months), of which 46.2% were female and 50.7% had a previous seizure history. The most frequent acute SE cause was a prolonged, complicated febrile seizure (20.6%). The most common initial seizure types were generalized seizures (49.9%), focal seizures (18.0%), and unknown types (12.1%); 40.5% of patients suffered from refractory SE and 5.0% from super-refractory SE. The three most common medications administered by nonmedically trained individuals were diazepam, midazolam, and antipyretics. The three most frequent anti-seizure medications (ASMs) administered by the emergency physician were midazolam, diazepam, and propofol. The three most common ASMs used in the clinical setting were midazolam, levetiracetam, and phenobarbital. New ASMs administered included lacosamide, brivaracetam, perampanel, stiripentol, and eslicarbazepine. Status epilepticus terminated in 16.0% in the preclinical setting, 19.1% in the emergency department, and 58.0% in the PICU; the outcome was unknown for 6.9%. The median PICU stay length was 2 (1-121) days. The median modified Rankin scale was 1 (0-5) on admission and 2 (0-6) at discharge. New neurological deficits after SE were observed in 6.2%. The mortality rate was 3.5%.
Significance: This study provides current real-world out-of- and in-hospital data on pediatric SE requiring PICU admission. New ASMs are more frequently used in this population. This knowledge may help generate a more standardized approach.
Keywords: anti-seizure medication.; diagnosis; follow-up; intensive care treatment; management; pediatric; seizure; status epilepticus; surveillance; therapy.
© 2023 The Authors. Epilepsia Open published by Wiley Periodicals LLC on behalf of International League Against Epilepsy.
Conflict of interest statement
This study received financial grants from the Dr. Wolf Epilepsy Project and Union Chimique Belge (UCB). Neither the Dr. Wolf Epilepsy Project nor UCB influenced the study design, data compilation, analysis, or presentation. Sascha Meyer reports research grants from Deutsche Forschungsgemeinschaft (DFG), UCB, Novartis, and the Dr. Wolf Epilepsy Project. Jaro Langer, Martin Poryo, Johannes Bay, Stefan Wagenpfeil, Beate Heinrich, and Holger Nunold report no financial support or conflicts of interest. Adam Strzelczyk reports personal fees and grants from Arvelle Therapeutics, Desitin Arzneimittel, Eisai, GW Pharmaceuticals, LivaNova, Marinus Pharma, Medtronic, UCB, and Zogenixs. Daniel Ebrahimi‐Fakhari reports research and travel grants from Tuberöse Sklerose Deutschland e.V. and personal fees from GW Pharmaceuticals.
Figures
References
-
- Raspall‐Chaure M, Chin RF, Neville BG, Scott RC. Outcome of paediatric convulsive status epilepticus: a systematic review. Lancet Neurol. 2006;5:769–79. - PubMed
-
- Chin RF, Neville BG, Peckham C, Bedford H, Wade A, Scott RC, et al. Incidence, cause, and short‐term outcome of convulsive status epilepticus in childhood: a prospective population‐based study. Lancet. 2006;368:222–9. - PubMed
-
- Pujar SS, Martinos MM, Cortina‐Borja M, Chong WKK, De Haan M, Gillberg C, et al. Long‐term prognosis after childhood convulsive status epilepticus: a prospective cohort study. Lancet Child Adolesc Health. 2018;2:103–11. - PubMed
-
- Cheng JY. Latency to treatment of status epilepticus is associated with mortality and functional status. J Neurol Sci. 2016;370:290–5. - PubMed
-
- Brophy GM, Bell R, Claassen J, Alldredge B, Bleck TP, Glauser T, et al. Guidelines for the evaluation and management of status epilepticus. Neurocrit Care. 2012;17:3–23. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
