

Chronic inflammatory demyelinating polyneuropathy caused by hepatocellular carcinoma
- PMID: 36764741
- PMCID: PMC9923304
- DOI: 10.1136/bcr-2022-251770
Chronic inflammatory demyelinating polyneuropathy caused by hepatocellular carcinoma
Abstract
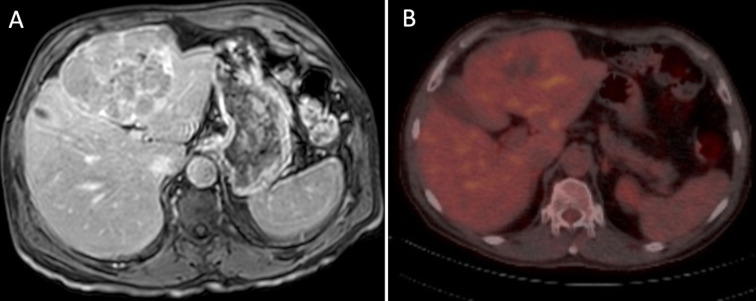
Paraneoplastic syndromes are rare abnormal endocrine or immune responses triggered by neoplasms. Chronic inflammatory demyelinating polyneuropathy (CIDP) is one such example. CIDP is an acquired, immune-mediated neuropathy affecting the peripheral nerves and nerve roots. It is associated with many types of cancers, especially haematological malignancies. We report the case of a man in his 60s who presented to the emergency department with acute symptoms of upper and lower extremity paresis and decreased sensation in the toes and tips of his fingers. Laboratory tests were normal. Electrodiagnostic studies showed diffuse motor and sensory dysfunction in all extremities; a diagnosis of CIDP was consequently made. Imaging studies showed a large left lobe liver mass. Subsequent biopsy revealed histopathological findings characteristic of hepatocellular carcinoma. After failure of medical treatment with intravenous immunoglobulin and corticosteroids, laparoscopic resection of the tumour was planned, performed and resulted in complete resolution of symptoms. At 18 months postoperatively, the patient was asymptomatic.
Keywords: liver disease; peripheral nerve disease; surgery.
© BMJ Publishing Group Limited 2023. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures


Similar articles
-
Association between chronic inflammatory demyelinating polyneuropathy and gastrointestinal malignancies.Clin J Gastroenterol. 2021 Feb;14(1):1-13. doi: 10.1007/s12328-020-01281-7. Epub 2020 Nov 4. Clin J Gastroenterol. 2021. PMID: 33146871 Review.
-
Chronic inflammatory demyelinating polyneuropathy following COVID-19 vaccination: a case report and literature review.BMC Neurol. 2024 Jul 29;24(1):262. doi: 10.1186/s12883-024-03756-3. BMC Neurol. 2024. PMID: 39075432 Free PMC article. Review.
-
Chronic inflammatory demyelinating polyradiculoneuropathy in a patient with systemic lupus erythematosus without systemic activity.Lupus. 2023 Aug;32(9):1123-1125. doi: 10.1177/09612033231186718. Epub 2023 Jun 27. Lupus. 2023. PMID: 37369195
-
Chronic inflammatory demyelinating polyradiculoneuropathy associated with Sjögren`s syndrome in a child.Turk J Pediatr. 2023;65(1):155-160. doi: 10.24953/turkjped.2022.460. Turk J Pediatr. 2023. PMID: 36866997
-
[Chronic inflammatory demyelinating polyneuropathy followed by systemic lupus erythematosus and Sjögren syndrome: a case report].Rinsho Shinkeigaku. 2006 Mar;46(3):203-9. Rinsho Shinkeigaku. 2006. PMID: 16642931 Japanese.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical