

Excessive Trabeculation of the Left Ventricle: JACC: Cardiovascular Imaging Expert Panel Paper
- PMID: 36764891
- PMCID: PMC9988693
- DOI: 10.1016/j.jcmg.2022.12.026
Excessive Trabeculation of the Left Ventricle: JACC: Cardiovascular Imaging Expert Panel Paper
Abstract
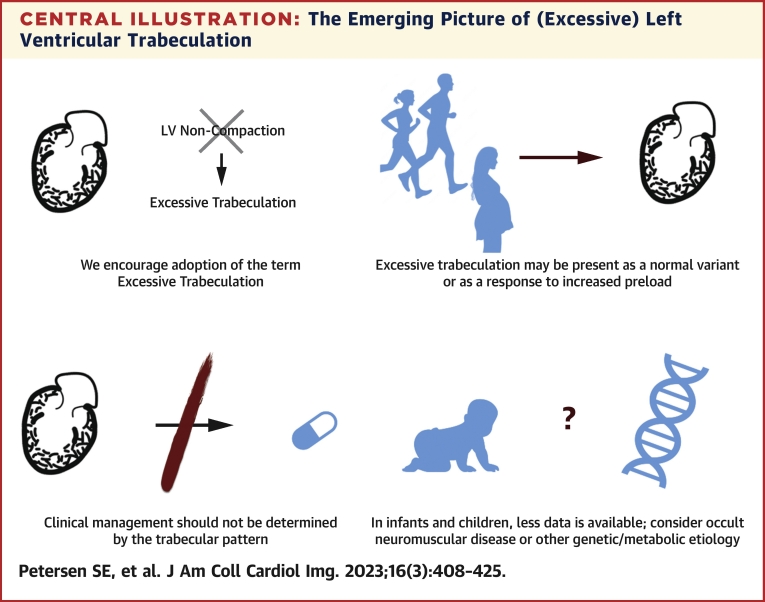
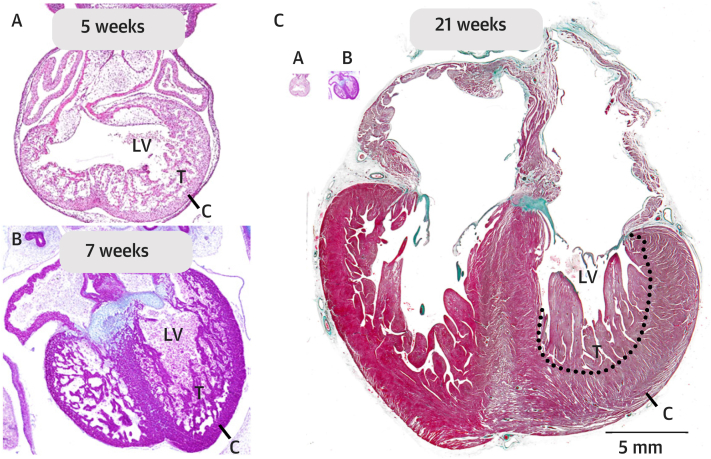
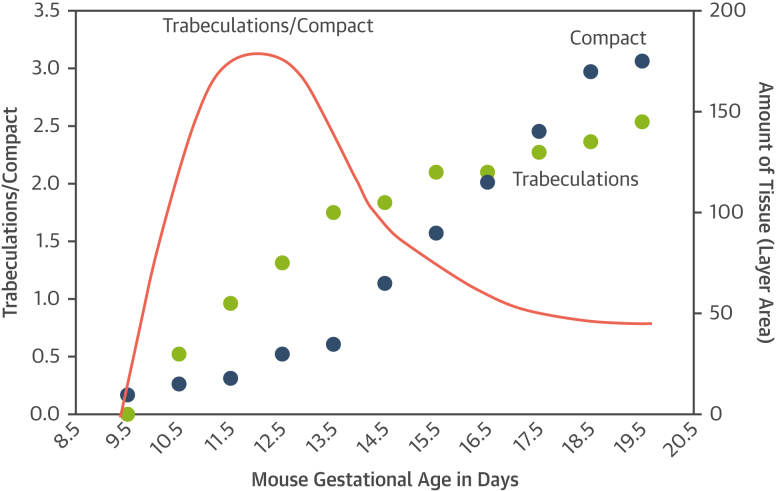
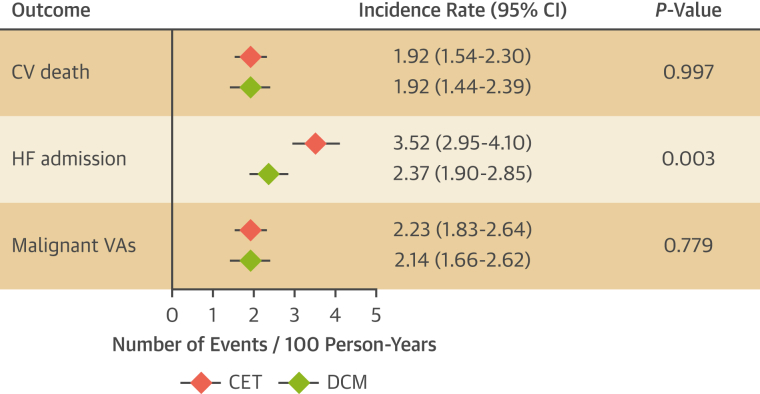
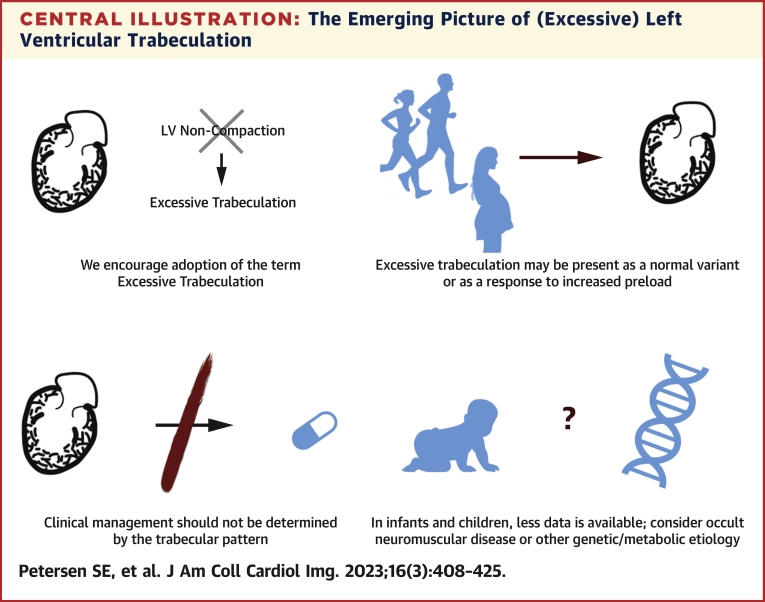
Excessive trabeculation, often referred to as "noncompacted" myocardium, has been described at all ages, from the fetus to the adult. Current evidence for myocardial development, however, does not support the formation of compact myocardium from noncompacted myocardium, nor the arrest of this process to result in so-called noncompaction. Excessive trabeculation is frequently observed by imaging studies in healthy individuals, as well as in association with pregnancy, athletic activity, and with cardiac diseases of inherited, acquired, developmental, or congenital origins. Adults with incidentally noted excessive trabeculation frequently require no further follow-up based on trabecular pattern alone. Patients with cardiomyopathy and excessive trabeculation are managed by cardiovascular symptoms rather than the trabecular pattern. To date, the prognostic role of excessive trabeculation in adults has not been shown to be independent of other myocardial disease. In neonates and children with excessive trabeculation and normal or abnormal function, clinical caution seems warranted because of the reported association with genetic and neuromuscular disorders. This report summarizes the evidence concerning the etiology, pathophysiology, and clinical relevance of excessive trabeculation. Gaps in current knowledge of the clinical relevance of excessive trabeculation are indicated, with priorities suggested for future research and improved diagnosis in adults and children.
Keywords: cardiovascular imaging; clinical management; diagnosis; etiology; left ventricular noncompaction; prognosis.
Copyright © 2023 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures Dr Petersen has received support from the National Institute for Health and Care Research Barts Biomedical Research Centre; and has consulted with Circle Cardiovascular Imaging Inc. Dr Friedrich has received support from the McGill Health Centre Foundation; has served as an advisor to and is a shareholder of Circle Cardiovascular Imaging Inc; and is a founder and shareholder of Area19 Medical Inc. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Discourage LVNC or Revise the Criteria of LVNC?JACC Cardiovasc Imaging. 2023 Jun;16(6):868. doi: 10.1016/j.jcmg.2023.03.024. JACC Cardiovasc Imaging. 2023. PMID: 37286273 No abstract available.
-
Reply: Discourage LVNC or Revise the Criteria of LVNC?JACC Cardiovasc Imaging. 2023 Jun;16(6):869. doi: 10.1016/j.jcmg.2023.03.023. JACC Cardiovasc Imaging. 2023. PMID: 37286274 No abstract available.
References
-
- Oechslin E., Jenni R. Left ventricular noncompaction: from physiologic remodeling to noncompaction cardiomyopathy. J Am Coll Cardiol. 2018;71(7):723–726. - PubMed
-
- Gati S., Chandra N., Bennett R.L., et al. Increased left ventricular trabeculation in highly trained athletes: do we need more stringent criteria for the diagnosis of left ventricular non-compaction in athletes? Heart. 2013;99(6):401–408. - PubMed
-
- Gati S., Papadakis M., Papamichael N.D., et al. Reversible de novo left ventricular trabeculations in pregnant women: implications for the diagnosis of left ventricular noncompaction in low-risk populations. Circulation. 2014;130(6):475–483. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
