

Epidemiology and outcomes of hospital-acquired bloodstream infections in intensive care unit patients: the EUROBACT-2 international cohort study
- PMID: 36764959
- PMCID: PMC9916499
- DOI: 10.1007/s00134-022-06944-2
Epidemiology and outcomes of hospital-acquired bloodstream infections in intensive care unit patients: the EUROBACT-2 international cohort study
Abstract
Purpose: In the critically ill, hospital-acquired bloodstream infections (HA-BSI) are associated with significant mortality. Granular data are required for optimizing management, and developing guidelines and clinical trials.
Methods: We carried out a prospective international cohort study of adult patients (≥ 18 years of age) with HA-BSI treated in intensive care units (ICUs) between June 2019 and February 2021.
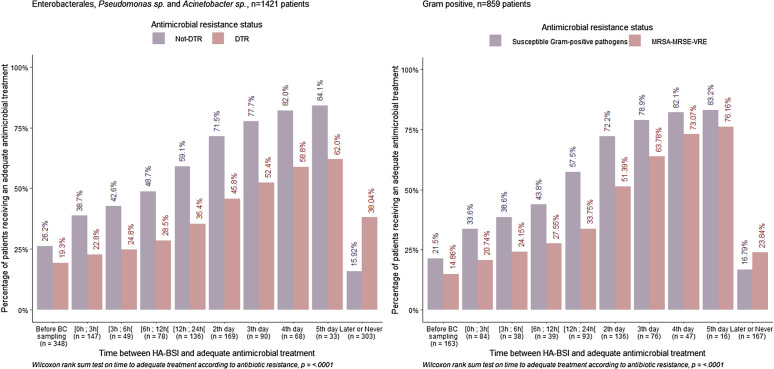
Results: 2600 patients from 333 ICUs in 52 countries were included. 78% HA-BSI were ICU-acquired. Median Sequential Organ Failure Assessment (SOFA) score was 8 [IQR 5; 11] at HA-BSI diagnosis. Most frequent sources of infection included pneumonia (26.7%) and intravascular catheters (26.4%). Most frequent pathogens were Gram-negative bacteria (59.0%), predominantly Klebsiella spp. (27.9%), Acinetobacter spp. (20.3%), Escherichia coli (15.8%), and Pseudomonas spp. (14.3%). Carbapenem resistance was present in 37.8%, 84.6%, 7.4%, and 33.2%, respectively. Difficult-to-treat resistance (DTR) was present in 23.5% and pan-drug resistance in 1.5%. Antimicrobial therapy was deemed adequate within 24 h for 51.5%. Antimicrobial resistance was associated with longer delays to adequate antimicrobial therapy. Source control was needed in 52.5% but not achieved in 18.2%. Mortality was 37.1%, and only 16.1% had been discharged alive from hospital by day-28.
Conclusions: HA-BSI was frequently caused by Gram-negative, carbapenem-resistant and DTR pathogens. Antimicrobial resistance led to delays in adequate antimicrobial therapy. Mortality was high, and at day-28 only a minority of the patients were discharged alive from the hospital. Prevention of antimicrobial resistance and focusing on adequate antimicrobial therapy and source control are important to optimize patient management and outcomes.
Keywords: antibiotic resistance; bacteremia; bloodstream infection; hospital-acquired.
© 2023. Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
AT has nothing to disclose, NB has nothing to disclose, QS has nothing to disclose, SR has nothing to disclose, MA reports honoraria paid to his university for educational activities by Pfizer, Sanofi, MSD and Astra Zeneca, ATA has nothing to disclose, ML reported consulting and lecture fees from Amomed Pharma, Aspen, LFB and Gilead, ACM has received payment for speaking on behalf of Boston Scientific and sits on the Scientific Advisory Board of Cambridge Infection Diagnostics, a start-up seeking to develop novel diagnostics for infectious diseases, MB received advisory board, speaker activities from Angelini, Bayer, Biomerieux, Cidara, Gilead, Menarini, MSD, Pfizer, Roche, Shionogi, study grants from: Angelini, Shionogi, Cidara, Gilead, Pfizer, and MSD, KA has nothing to disclose, JL has received lecture fees and honoraria from MSD, RF reports Payment for lectures, speakers bureaus or advisory boards from Grifols, MSD, Pfizer, Gilead, Shionogi, Thermofisher, Hill Rom, AOP Health, BD, HQ has nothing to disclose, JAP reports consulting, advisory boards or lectures fees and honoraria for MSD, Pfizer, Astra-Zeneca, Gilead, Jansen, Cepheid, AOP Orphan Pharmaceuticals, PP reported advisory boards participation for Gilead, Technophage and Sanofi, lectures fees from MSD, Gilead and Pfizer, and research grant from Abionic, LDB has nothing to disclose, JdW has consulted for Pfizer, MSD (honoraria paid to institution), FZ has nothing to disclose, MG has nothing to disclose, AA has nothing to disclose, KA has nothing to disclose, HB has nothing to disclose, YH has nothing to disclose, KJ has nothing to disclose, ME has nothing to disclose, FB reported consulting and lecture fees, conference invitation from MSD and lecture fees from BioMérieux, J-FT reported advisory boards participation for Merck, Gilead, Beckton-Dickinson, Pfizer, Shinogi, Medimune, Paratek, research grants from Merck, Pfizer, Thermofischer.
Figures
References
-
- Cassini A, Plachouras D, Eckmanns T, Abu Sin M, Blank H-P, Ducomble T, et al. Burden of six healthcare-associated infections on European population health: estimating incidence-based disability-adjusted life years through a population prevalence-based modelling study. PLoS Med. 2016;13(10):e1002150. doi: 10.1371/journal.pmed.1002150. - DOI - PMC - PubMed
-
- Tabah A, Koulenti D, Laupland K, Misset B, Valles J, Bruzzi de Carvalho F, et al. Characteristics and determinants of outcome of hospital-acquired bloodstream infections in intensive care units: the EUROBACT International Cohort Study. Intensive Care Med. 2012;38(12):1930–1945. doi: 10.1007/s00134-012-2695-9. - DOI - PubMed
-
- Adrie C, Garrouste-Orgeas M, Ibn Essaied W, Schwebel C, Darmon M, Mourvillier B, et al. Attributable mortality of ICU-acquired bloodstream infections: impact of the source, causative micro-organism, resistance profile and antimicrobial therapy. J Infect. 2017;74(2):131–141. doi: 10.1016/j.jinf.2016.11.001. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
