

Cellular angiofibroma in the retroperitoneal space during pregnancy: A case report
- PMID: 36765343
- PMCID: PMC9912601
- DOI: 10.1186/s12905-023-02182-w
Cellular angiofibroma in the retroperitoneal space during pregnancy: A case report
Abstract
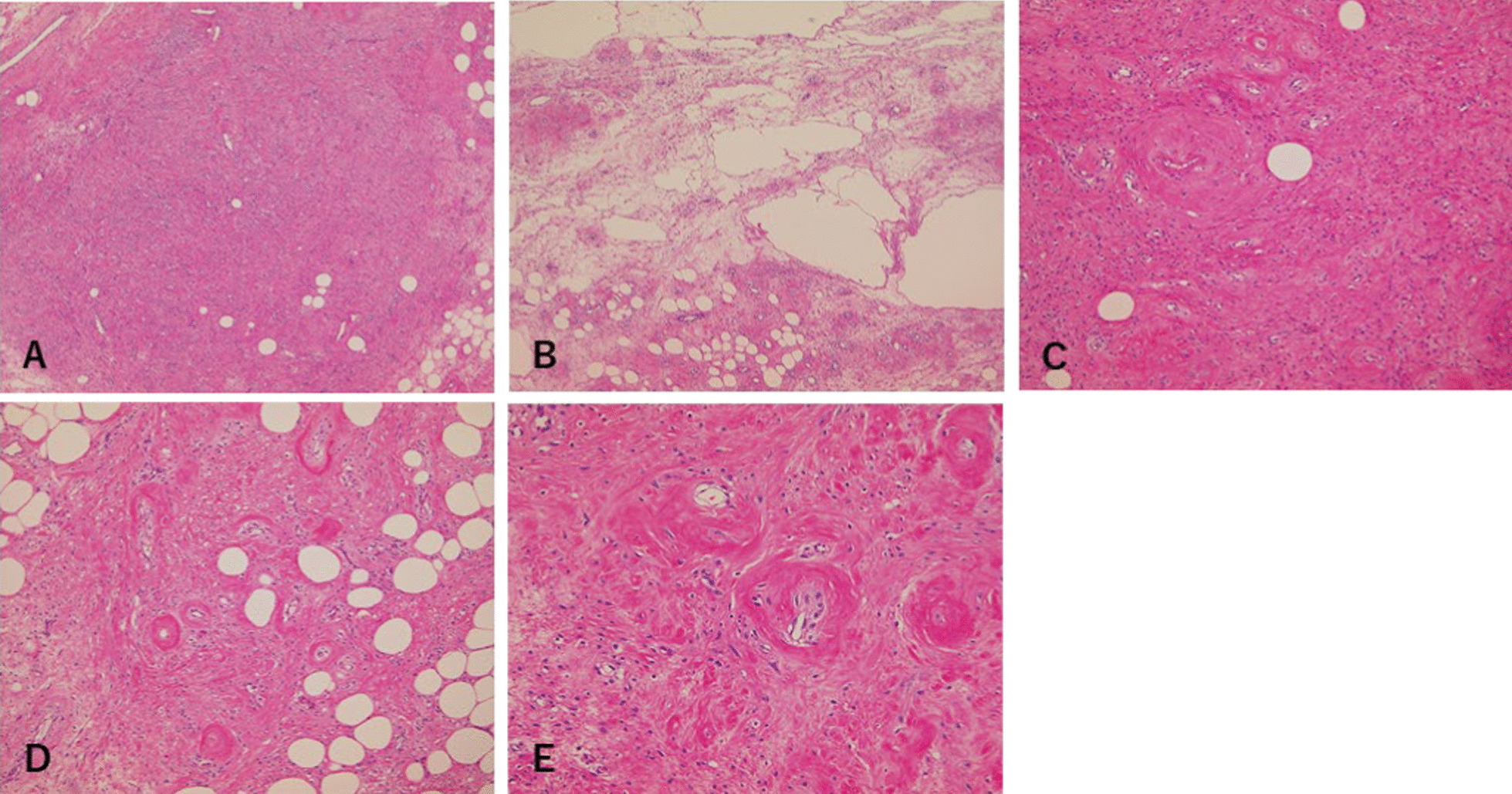
Background: Cellular angiofibroma (CA) is a rare, benign mesenchymal tumor first described by Nucci et al. (Am J Surg Pathol 21:636-644, 1997. 10.1097/00000478-199706000-00002). It affects both men and women, although it is more common in middle-aged women. CA is well circumscribed and usually observed on the body surface, primarily in distal genital regions. Aggressive angiomyxoma and angiomyofibroblastoma are clinically and histologically similar; therefore, it may be necessary to distinguish between CA and these similar tumors. We present a rare case of CA, with atypical features, in the retroperitoneal space during pregnancy.
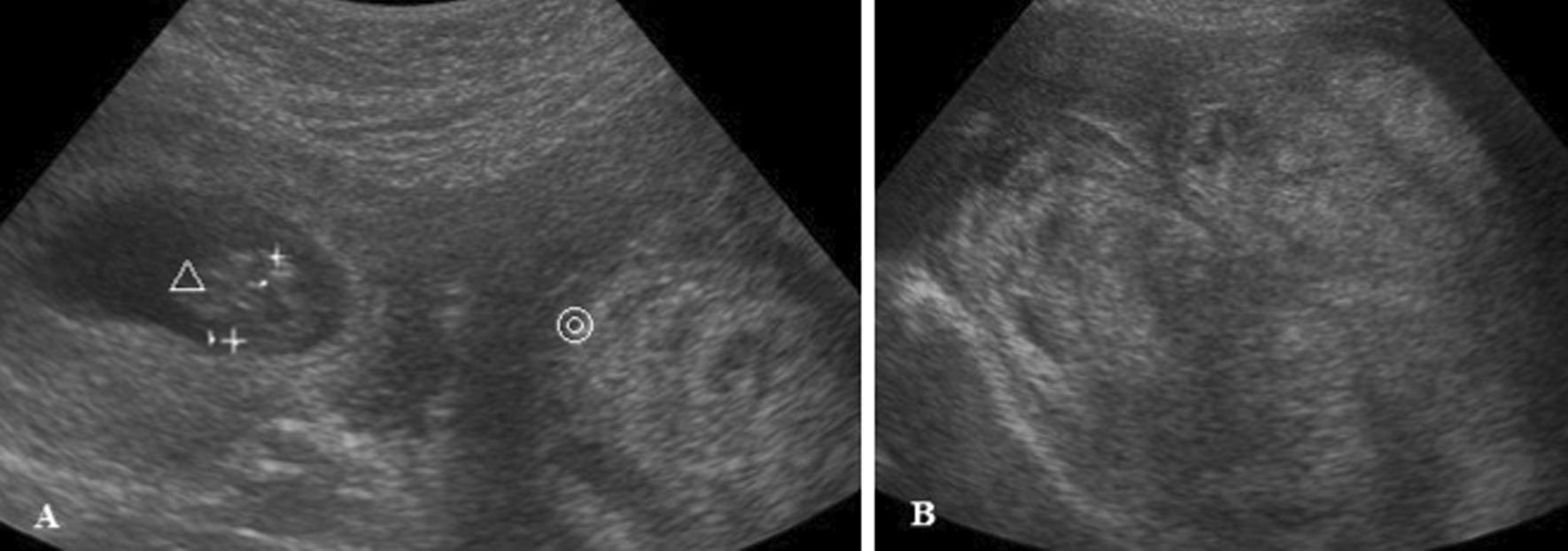
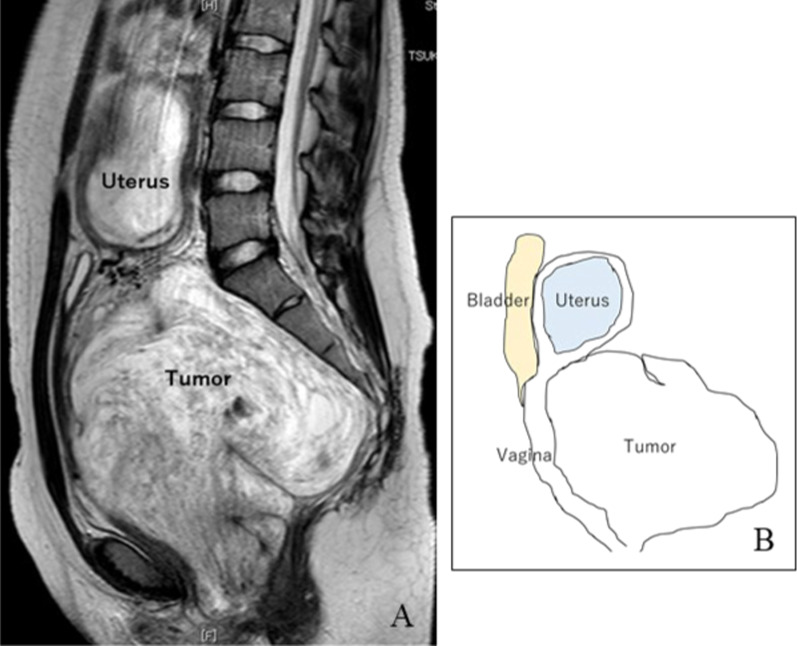
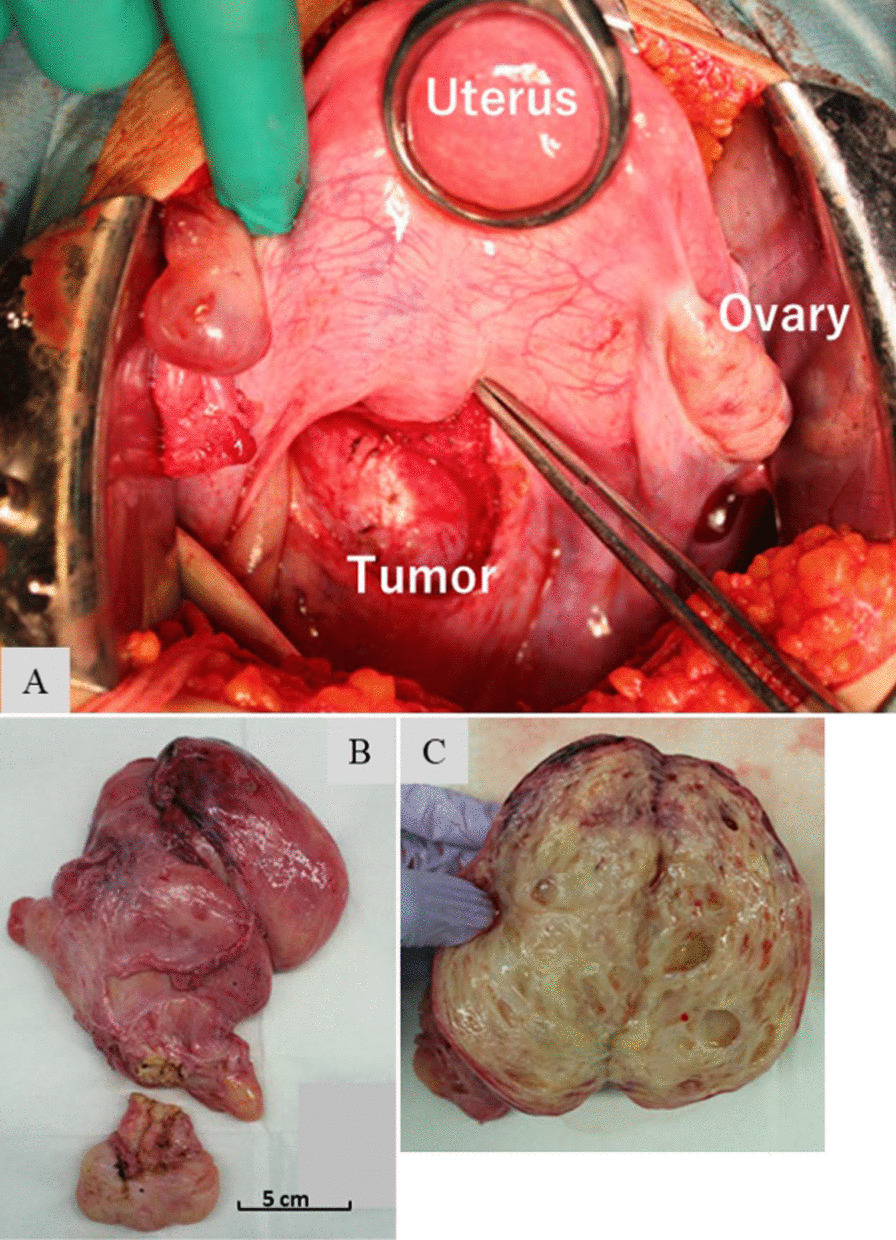
Case presentation: The presence of a 130 mm tumor was detected in a 19-year-old woman. The tumor, located in the retroperitoneal space, was found during first pregnancy examination. At 16 weeks of gestation, the woman developed nausea and fever, and it was diagnosed with acute pyelonephritis. After a few days, the amniotic membranes prematurely ruptured, leading to a miscarriage. The woman underwent a tumor resection, after miscarriage. This case presented with atypical features of CA. This included the young age of the patient, and presence of a tumor in the retroperitoneal space.
Conclusion: In this case, the diagnosis of CA was difficult due to the rarity of the disease and its atypical clinical features. From this experience, we recommend that the discussion on the efficacy of surgical treatment and pregnancy outcomes should be done based on individual case, and not generalized.
Keywords: Aggressive angiomyxoma; Angiomyofibroblastoma; Cellular angiofibroma; Intraperitoneal space; Pregnancy.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
