

De-Implementing Opioids for Dental Extractions (DIODE): a multi-clinic, cluster-randomized trial of clinical decision support strategies in dentistry
- PMID: 36765414
- PMCID: PMC9913004
- DOI: 10.1186/s13012-023-01262-7
De-Implementing Opioids for Dental Extractions (DIODE): a multi-clinic, cluster-randomized trial of clinical decision support strategies in dentistry
Abstract
Background: Opioid pain relievers are commonly prescribed following dental extractions, but evidence shows that non-opioid analgesics often provide adequate pain relief with fewer risks. The current study examined clinical decision support (CDS) as a tool for de-implementing opioid prescribing in dentistry.
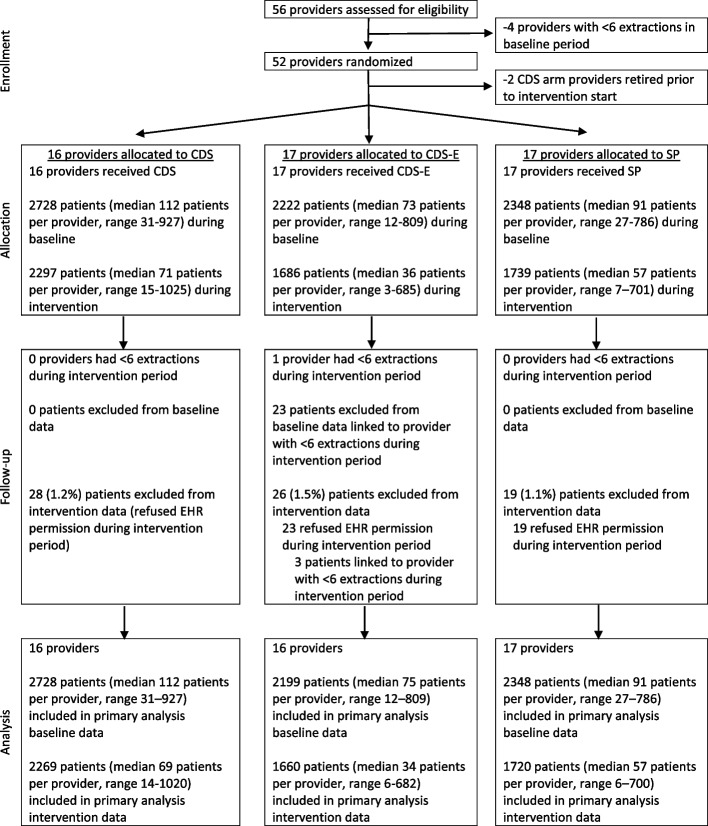
Methods: This prospective, cluster-randomized trial examined CDS for dental pain management at 22 HealthPartners Dental Group clinics in Minnesota. Dental providers (n = 49) were randomized to deliver care using CDS, CDS with patient education materials (CDS-E), or standard practice (SP). Randomization was stratified by provider type (dentist vs. oral surgeon) and baseline opioid prescribing volume. Patient records of dental extractions were examined for January 2019 through May 2021, representing a 12-month baseline and 15-month intervention period (N = 12,924). Opioid prescription at the visit (no vs. yes) was the primary outcome. Data were analyzed using generalized linear mixed models, adjusting for patient sex and age, extraction complexity, and baseline prescribing strata (volume and provider type).
Results: Patients were 56.2% female, with a mean age of 46.7 (SD = 20.0) years. Providers were 8% oral surgeons, 57% female, and with a mean age of 43.7 (SD = 11.2) years. There were significant decreases in opioid prescribing during the study (P < 0.001), representing a continuation of pre-existing trends to reduce opioid prescribing in these dental practices. There were no significant differences in opioid prescribing between CDS and SP (OR = 1.29; 97.5% CI = 0.93, 1.79; P = 0.08), or CDS-E and SP arms (OR = 1.27; 97.5% CI = 0.86, 1.79; P = 0.18). The direction of the association favored greater reductions in opioid prescribing in the SP arm. Despite training and implementation support, utilization of the CDS was low, particularly among oral surgeons, who were significantly more likely than other dentists to prescribe opioids. Among non-oral surgeon providers with the opportunity to access it, CDS utilization was not significantly associated with opioid prescribing.
Conclusions: Equipping dentists with CDS resources, whether alone or accompanied by patient education materials, did not accelerate reductions in opioid prescribing beyond those observed in standard practice. Strategies are needed to enhance CDS utilization for patient care and safety surrounding analgesia following dental extractions.
Trial registration: Clinicaltrials.gov, NCT03584789.
Keywords: Clinical decision support; De-implementation; Dentistry; Opioids.
© 2023. The Author(s).
Conflict of interest statement
Unrelated to the present study, JG is part owner of COG Analytics and has received donated study medication from Indivior and Alkermes as part of NIH-funded research. Unrelated to the present study, SGM is co-PI on a NIDA study that was provided medication in-kind by Braeburn.
Figures
References
-
- CDC . Drug overdose deaths in the U.S. top 100,000 annually. 2021.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
