

Risk Group Stratification for Recurrence-Free Survival and Early Tumor Recurrence after Radiofrequency Ablation for Hepatocellular Carcinoma
- PMID: 36765645
- PMCID: PMC9913840
- DOI: 10.3390/cancers15030687
Risk Group Stratification for Recurrence-Free Survival and Early Tumor Recurrence after Radiofrequency Ablation for Hepatocellular Carcinoma
Abstract
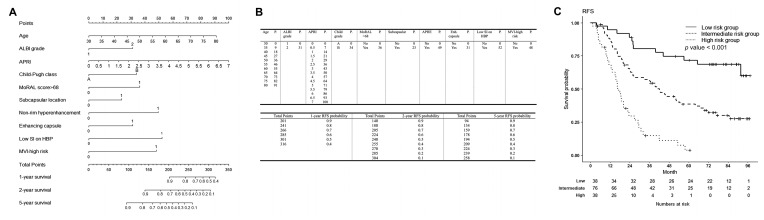
Purpose: Although the prognosis after radiofrequency ablation (RFA) for hepatocellular carcinoma (HCC) may vary according to different risk levels, there is no standardized follow-up protocol according to each patient's risk. This study aimed to stratify patients according to their risk of recurrence-free survival (RFS) and early (≤2 years) tumor recurrence (ETR) after RFA for HCC based on predictive models and nomograms and to compare the survival times of the risk groups derived from the models.
Methods: Patients who underwent RFA for a single HCC (≤3 cm) between January 2012 and March 2014 (n = 152) were retrospectively reviewed. Patients were classified into low-, intermediate-, and high-risk groups based on the total nomogram points for RFS and ETR, respectively, and compared for each outcome. Restricted mean survival times (RMSTs) in the three risk groups were evaluated for both RFS and ETR to quantitatively evaluate the difference in survival times.
Results: Predictive models for RFS and ETR were constructed with c-indices of 0.704 and 0.730, respectively. The high- and intermediate-risk groups for RFS had an 8.5-fold and 2.9-fold higher risk of events than the low-risk group (both p < 0.001), respectively. The high- and intermediate-risk groups for ETR had a 17.7-fold and 7.0-fold higher risk than the low-risk group (both p < 0.001), respectively. The RMST in the high-risk group was significantly lower than that in the other two groups 9 months after RFA, and that in the intermediate-risk group became lower than that in the low-risk group after 21 months with RFS and 24 months with ETR.
Conclusion: Our predictive models were able to stratify patients into three groups according to their risk of RFS and ETR after RFA for HCC. Differences in RMSTs may be used to establish different follow-up protocols for the three risk groups.
Keywords: carcinoma; hepatocellular; nomogram; predictive model; prognosis; radiofrequency ablation; survival times.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
-
- Marrero J.A., Kulik L.M., Sirlin C.B., Zhu A.X., Finn R.S., Abecassis M.M., Roberts L.R., Heimbach J.K. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology. 2018;68:723–750. doi: 10.1002/hep.29913. - DOI - PubMed
-
- Rossi S., Ravetta V., Rosa L., Ghittoni G., Viera F.T., Garbagnati F., Silini E.M., Dionigi P., Calliada F., Quaretti P., et al. Repeated radiofrequency ablation for management of patients with cirrhosis with small hepatocellular carcinomas: A long-term cohort study. Hepatology. 2011;53:136–147. doi: 10.1002/hep.23965. - DOI - PubMed
-
- Shiina S., Tateishi R., Arano T., Uchino K., Enooku K., Nakagawa H., Asaoka Y., Sato T., Masuzaki R., Kondo Y., et al. Radiofrequency ablation for hepatocellular carcinoma: 10-year outcome and prognostic factors. Am. J. Gastroenterol. 2012;107:569–577. doi: 10.1038/ajg.2011.425. quiz 578. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
