

SAINT: A Phase I/Expanded Phase II Study Using Safe Amounts of Ipilimumab, Nivolumab and Trabectedin as First-Line Treatment of Advanced Soft Tissue Sarcoma
- PMID: 36765863
- PMCID: PMC9913367
- DOI: 10.3390/cancers15030906
SAINT: A Phase I/Expanded Phase II Study Using Safe Amounts of Ipilimumab, Nivolumab and Trabectedin as First-Line Treatment of Advanced Soft Tissue Sarcoma
Abstract
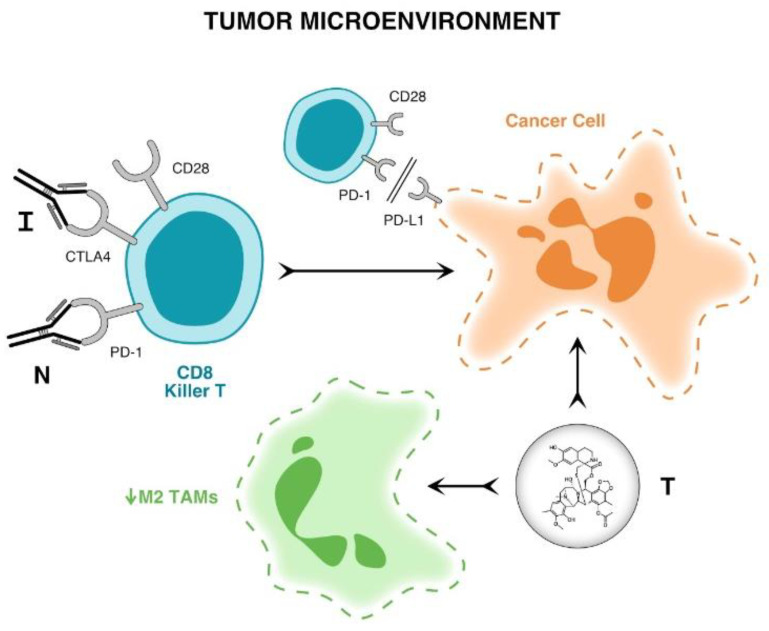
Background: This Phase 1/2 study is based on the hypothesis that immune checkpoint inhibitors are more effective when given earlier in the course of the disease for advanced soft tissue sarcoma.
Methods: Phase I endpoints-maximum tolerated dose in previously treated patients; Phase II endpoints-best response, progression free survival and overall survival and incidence of adverse events in previously untreated patients; Phase I treatments-escalating doses of trabectedin (1.0, 1.2, 1.5 mg/m2) as continuous intravenous infusion over 24 h every 3 weeks, 1 mg/kg of ipilimumab given intravenously every 12 weeks, and 3 mg/kg of nivolumab given intravenously every 2 weeks; Phase II treatments-maximum tolerated dose of trabectedin and defined doses of ipilimumab and nivolumab.
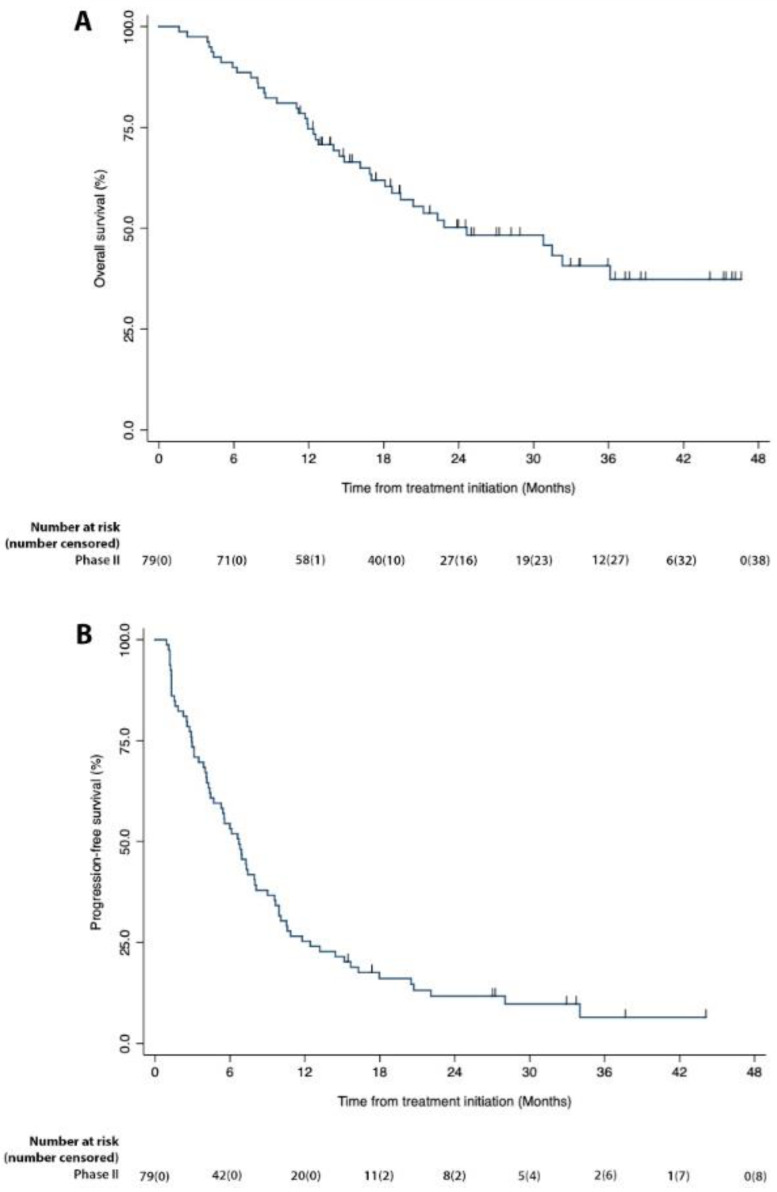
Results: Phase I (n = 9)-the maximum tolerated dose of trabectedin was 1.2 mg/m2; Phase II (n = 79)-6 complete responses, 14 partial responses, 49 stable disease, 25.3% best response rate, 87.3% disease control rate; median progression-free survival, 6.7 months (CI 95%: 4.4-7.9), median overall survival, 24.6 months (CI 95%: 17.0-.); Grade 3/4 therapy-related adverse events (n = 92)-increased ALT (25%), fatigue (8.7%), increased AST (8.7%), decreased neutrophil count (5.4%) and anemia (4.6%).
Conclusion: SAINT is a safe and effective first-line treatment for advanced soft tissue sarcoma.
Keywords: alkylating agent; chemotherapy; immune checkpoint inhibitor; immunotherapy; ipilimumab; nivolumab and trabectedin; soft tissue sarcoma.
Conflict of interest statement
The authors E.M.G., S.P.C., W.A.T., E.Y., S.T., V.S.C.-A., H.C., C.V., D.A.B., A.M., S.G.W., D.Q., A.S., N.F., W.T. have no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures
References
-
- Wagner M.J., Ismaila L., Duh M., Korves C., Solleza F., Manson S., Diaz J., Neary M., Demetri G. A retrospective chart review of drug treatment patterns and clinical outcomes among patients with metastatic or recurrent soft tissue sarcoma refractory to one or more prior chemotherapy treatments. BMC Cancer. 2015;15:175. doi: 10.1186/s12885-015-1182-4. - DOI - PMC - PubMed
-
- Judson I., Verweij J., Gelderblom H., Hartmann J.T., Schöffski P., Blay J.Y., Kerst J.M., Sufliarsky J., Whelan J., Hohenberger P., et al. Doxorubicin alone versus intensified doxorubicin plus ifosfamide for firstline treatment of advanced or metastatic soft-tissue sarcoma: A randomised controlled phase 3 trial. Lancet Oncol. 2014;15:415–423. doi: 10.1016/S1470-2045(14)70063-4. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Medical
