

Radiofrequency Ablation, Cryoablation, and Microwave Ablation for the Treatment of Small Renal Masses: Efficacy and Complications
- PMID: 36766493
- PMCID: PMC9914157
- DOI: 10.3390/diagnostics13030388
Radiofrequency Ablation, Cryoablation, and Microwave Ablation for the Treatment of Small Renal Masses: Efficacy and Complications
Abstract
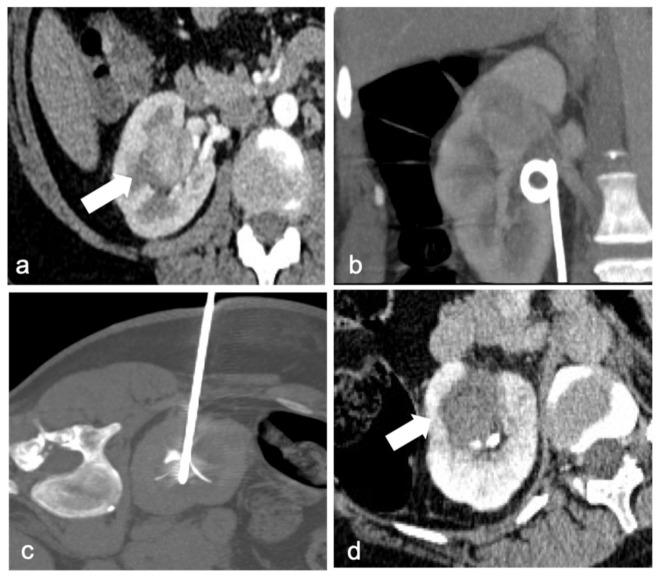
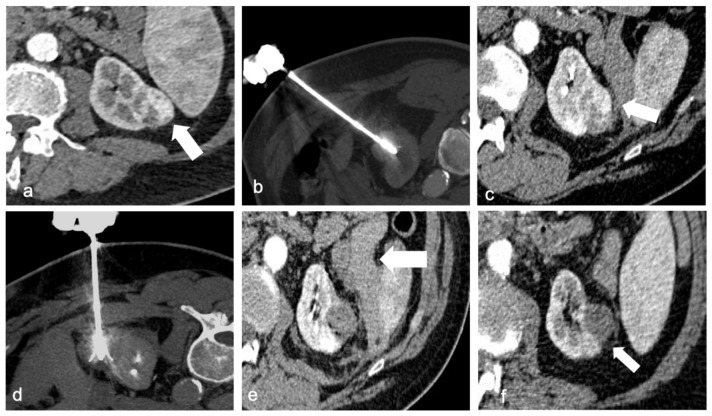
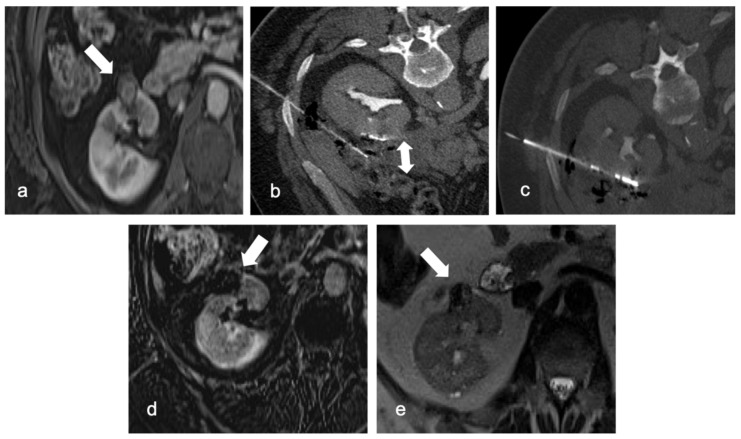
Over the last two decades the detection rate of small renal masses has increased, due to improving diagnostic accuracy, and nephron-sparing treatments have become the first-choice curative option for small renal masses. As a minimally invasive alternative, thermal ablation has increased in popularity, offering a good clinical outcome and low recurrence rate. Radiofrequency ablation, Cryoablation, and Microwave ablation are the main ablative techniques. All of them are mostly overlapping in term of cancer specific free survival and outcomes. These techniques require imaging study to assess lesions features and to plan the procedure: US, CT, and both of them together are the leading guidance alternatives. Imaging findings guide the interventional radiologist in assessing the risk of complication and possible residual disease after procedure. The purpose of this review is to compare different ablative modalities and different imaging guides, underlining the effectiveness, outcomes, and complications related to each of them, in order to assist the interventional radiologist in choosing the best option for the patient.
Keywords: ablation; imaging guide; renal cell carcinoma (RCC); small renal masses.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Ljungberg B., Albiges L., Abu-Ghanem Y., Bedke J., Capitanio U., Dabestani S., Fernández-Pello S., Giles R.H., Hofmann F., Hora M., et al. European Association of Urology Guidelines on Renal Cell Carcinoma: The 2022 Update. Eur. Urol. 2022;82:399–410. doi: 10.1016/j.eururo.2022.03.006. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
