

Diagnostic Utility of Double-Echo Steady-State (DESS) MRI for Fracture and Bone Marrow Edema Detection in Adolescent Lumbar Spondylolysis
- PMID: 36766566
- PMCID: PMC9914111
- DOI: 10.3390/diagnostics13030461
Diagnostic Utility of Double-Echo Steady-State (DESS) MRI for Fracture and Bone Marrow Edema Detection in Adolescent Lumbar Spondylolysis
Abstract
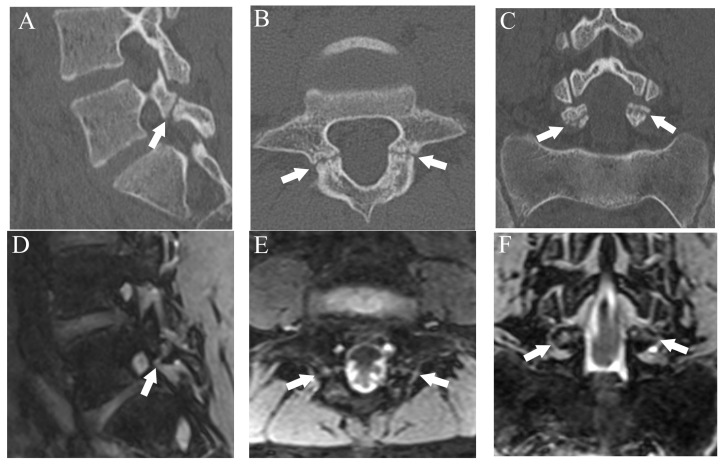
To evaluate the ability of double-echo steady-state (DESS) MRI to detect pars interarticularis fracture and bone marrow edema (BME) in spondylolysis, 500 lumber pars interarticularis from 50 consecutive patients (38 males and 12 females, mean age 14.2 ± 3.28 years) with spondylolysis who underwent both MRI and CT within 1 week were evaluated. All participants were young athletes who complained of lower back pain. Fractures were classified into four grades and CT was used as a reference; BME was evaluated in a binary manner and STIR was used as a reference. The diagnostic performance of fractures on DESS and T1WI, and BME on DESS was assessed by two radiologists independently. For fracture detection, DESS showed high diagnostic performance at a sensitivity of 94%, specificity of 99.5%, and accuracy of 98.8%, whereas T1WI showed lower sensitivity (70.1%). Fracture grading performed by DESS showed excellent agreement with CT grading (Kappa = 0.9). For BME, the sensitivity, specificity, and accuracy of DESS were 96.5%, 100%, and 99.6%, respectively. The inter-rater agreement of DESS for fracture and BME was 0.8 and 0.85, respectively. However, the inter-rater agreement for fracture on T1WI was 0.52. DESS had high diagnostic performance for fracture and BME in pars interarticularis. In conclusion, DESS had potential to detect all critical imaging findings in spondylolysis and may replace the role of CT.
Keywords: bone marrow edema; computed tomography; fracture; magnetic resonance imaging; pars interarticularis; spondylolysis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures






References
LinkOut - more resources
Full Text Sources
Miscellaneous
