

Early Surfactant Therapy for Respiratory Distress Syndrome in Very Preterm Infants
- PMID: 36767013
- PMCID: PMC9914192
- DOI: 10.3390/healthcare11030439
Early Surfactant Therapy for Respiratory Distress Syndrome in Very Preterm Infants
Abstract
Background: It is currently considered that early initiation of nasal continuous positive airway pressure, using a less invasive exogenous surfactant administration and avoiding mechanical ventilation as much as possible to minimize lung damage, may reduce mortality and/or the risk of morbidities in preterm infants. The aim of our study was to quantify our experience and compare different strategies of surfactant administration, to investigate which method is associated with less morbidity.
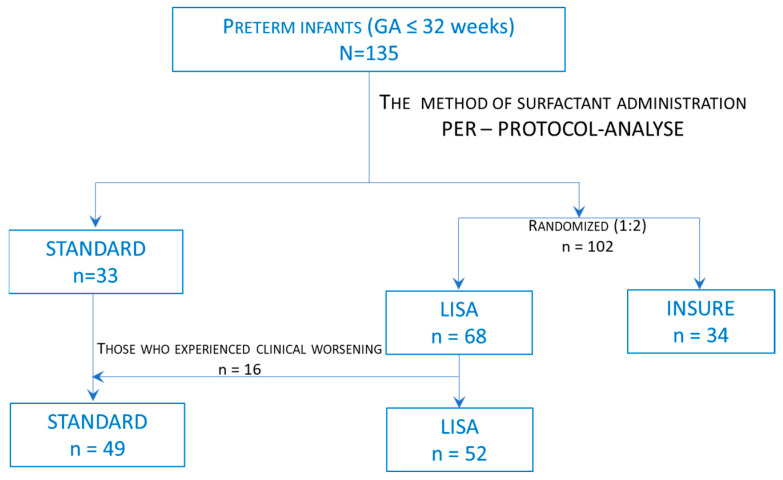
Materials and methods: A total of 135 preterm infants with early rescue surfactant administration for respiratory distress syndrome were included in the study. The infants were treated in an academic, Level III Neonatal Intensive Care Unit over a 3-year period between 1 December 2018 and 1 December 2021. Patients were separated into three groups: those with standard surfactant administration; those with Less Invasive Surfactant Administration-LISA; and those with Intubation Surfactant Administration Extubation-INSURE. As a primary outcome, we followed the need for intubation and mechanical ventilation within 72 h, while the secondary outcomes were major neonatal morbidities and death before discharge.
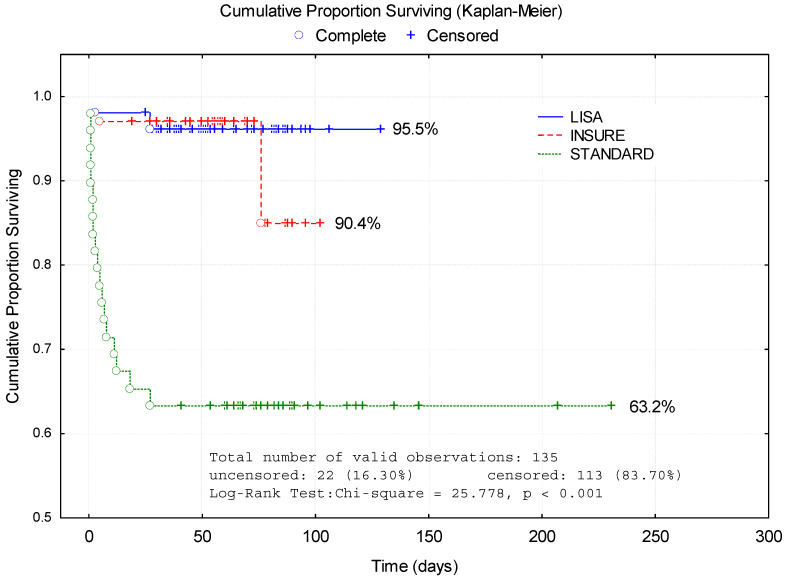
Results: The surfactant administration method was significantly associated with the need for mechanical ventilation within 72 h after the procedure (p < 0.001). LISA group infants needed less MV (OR = 0.538, p = 0.019) than INSURE group infants. We found less morbidities (OR = 0.492, p = 0.015) and deaths before discharge (OR = 0.640, p = 0.035) in the LISA group compared with the INSURE group. The analysis of morbidities found in infants who were given the surfactant by the LISA method compared with the INSURE method showed lower incidence of pneumothorax (3.9% vs. 8.8%), intraventricular hemorrhage (17.3% vs. 23.5%), intraventricular hemorrhage grade 3 and 4 (3.9% vs. 5.9%), sepsis/probable sepsis (11.5% vs. 17.7%) retinopathy of prematurity (16.7% vs. 26.7%) and deaths (3.9% vs. 5.9%). There were no significant differences between groups in frequencies of bronchopulmonary dysplasia, necrotizing enterocolitis and patent ductus arteriosus.
Conclusions: Less invasive surfactant administration methods seem to have advantages regarding early need for mechanical ventilation, decreasing morbidities and death rate. In our opinion, the LISA procedure may be a good choice in spontaneously breathing infants regardless of gestational age.
Keywords: INSURE; LISA; preterm infant; respiratory distress syndrome; surfactant.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
