

DSP-Related Cardiomyopathy as a Distinct Clinical Entity? Emerging Evidence from an Italian Cohort
- PMID: 36768812
- PMCID: PMC9916412
- DOI: 10.3390/ijms24032490
DSP-Related Cardiomyopathy as a Distinct Clinical Entity? Emerging Evidence from an Italian Cohort
Abstract
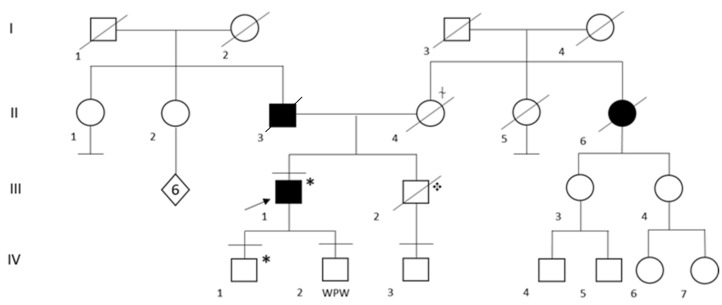
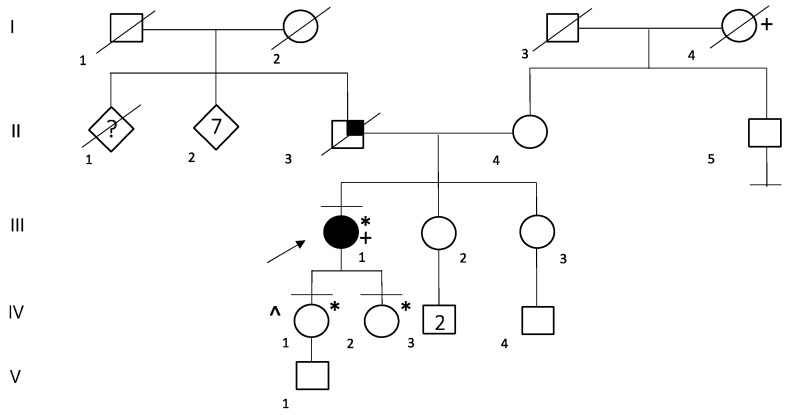
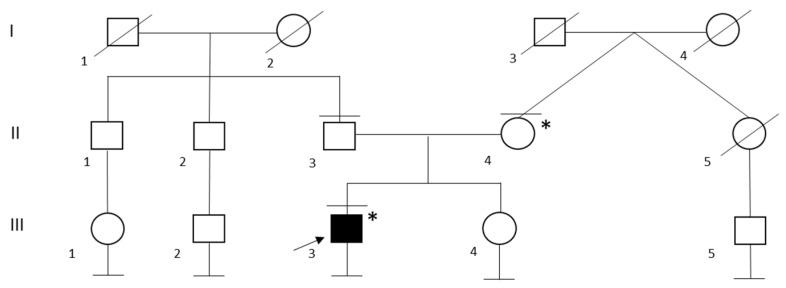
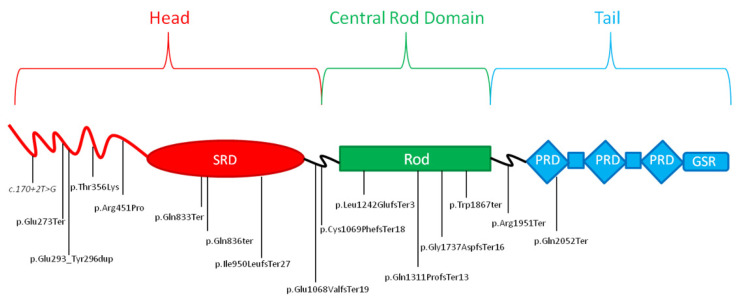
Variants in desmoplakin gene (DSP MIM *125647) have been usually associated with Arrhythmogenic Cardiomyopathy (ACM), or Dilated Cardiomyopathy (DCM) inherited in an autosomal dominant manner. A cohort of 18 probands, characterized as heterozygotes for DSP variants by a target Next Generation Sequencing (NGS) cardiomyopathy panel, was analyzed. Cardiological, genetic data, and imaging features were retrospectively collected. A total of 16 DSP heterozygous pathogenic or likely pathogenic variants were identified, 75% (n = 12) truncating variants, n = 2 missense variants, n = 1 splicing variant, and n = 1 duplication variant. The mean age at diagnosis was 40.61 years (IQR 31-47.25), 61% of patients being asymptomatic (n = 11, New York Heart Association (NYHA) class I) and 39% mildly symptomatic (n = 7, NYHA class II). Notably, 39% of patients (n = 7) presented with a clinical history of presumed myocarditis episodes, characterized by chest pain, myocardial enzyme release, 12-lead electrocardiogram abnormalities with normal coronary arteries, which were recurrent in 57% of cases (n = 4). About half of the patients (55%, n = 10) presented with a varied degree of left ventricular enlargement (LVE), four showing biventricular involvement. Eleven patients (61%) underwent implantable cardioverter defibrillator (ICD) implantation, with a mean age of 46.81 years (IQR 36.00-64.00). Cardiac magnetic resonance imaging (CMRI) identified in all 18 patients a delayed enhancement (DE) area consistent with left ventricular (LV) myocardial fibrosis, with a larger localization and extent in patients presenting with recurrent episodes of myocardial injury. These clinical and genetic data confirm that DSP-related cardiomyopathy may represent a distinct clinical entity characterized by a high arrhythmic burden, variable degrees of LVE, Late Gadolinium Enhancement (LGE) with subepicardial distribution and episodes of myocarditis-like picture.
Keywords: arrhythmogenic cardiomyopathy; desmoplakin; dilated cardiomyopathy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Corrado D., van Tintelen P.J., McKenna W.J., Hauer R.N.W., Anastastakis A., Asimaki A., Basso C., Bauce B., Brunckhorst C., Bucciarelli-Ducci C., et al. Arrhythmogenic right ventricular cardiomyopathy: Evaluation of the current diagnostic criteria and differential diagnosis. Eur. Heart J. 2020;41:1414–1429. doi: 10.1093/eurheartj/ehz669. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
