

CD4 T-Cell Subsets and the Pathophysiology of Inflammatory Bowel Disease
- PMID: 36769019
- PMCID: PMC9916759
- DOI: 10.3390/ijms24032696
CD4 T-Cell Subsets and the Pathophysiology of Inflammatory Bowel Disease
Abstract
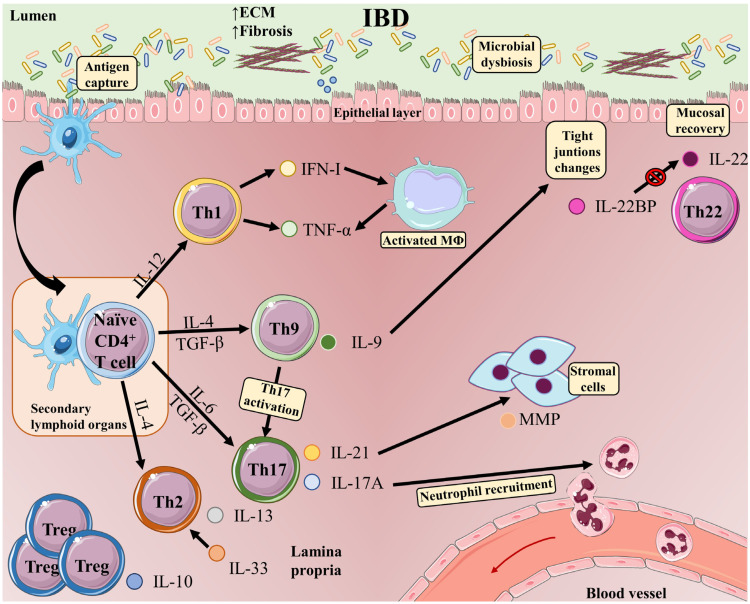
Inflammatory bowel disease (IBD) is an umbrella term for the chronic immune-mediated idiopathic inflammation of the gastrointestinal tract, manifesting as Crohn's disease (CD) or ulcerative colitis (UC). IBD is characterized by exacerbated innate and adaptive immunity in the gut in association with microbiota dysbiosis and the disruption of the intestinal barrier, resulting in increased bacterial exposure. In response to signals from microorganisms and damaged tissue, innate immune cells produce inflammatory cytokines and factors that stimulate T and B cells of the adaptive immune system, and a prominent characteristic of IBD patients is the accumulation of inflammatory T-cells and their proinflammatory-associated cytokines in intestinal tissue. Upon antigen recognition and activation, CD4 T-cells differentiate towards a range of distinct phenotypes: T helper(h)1, Th2, Th9, Th17, Th22, T follicular helper (Tfh), and several types of T-regulatory cells (Treg). T-cells are generated according to and adapt to microenvironmental conditions and participate in a complex network of interactions among other immune cells that modulate the further progression of IBD. This review examines the role of the CD4 T-cells most relevant to IBD, highlighting how these cells adapt to the environment and interact with other cell populations to promote or inhibit the development of IBD.
Keywords: Crohn’s disease; Th1; Th17; Th19; Th2; Th22; Treg; adaptive immune system; inflammatory bowel disease; regulatory T-cell; ulcerative colitis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
