

Factors Associated with Progression of Atrial Fibrillation and Impact on All-Cause Mortality in a Cohort of European Patients
- PMID: 36769416
- PMCID: PMC9917523
- DOI: 10.3390/jcm12030768
Factors Associated with Progression of Atrial Fibrillation and Impact on All-Cause Mortality in a Cohort of European Patients
Abstract
Background: Paroxysmal atrial fibrillation (AF) may often progress towards more sustained forms of the arrhythmia, but further research is needed on the factors associated with this clinical course.
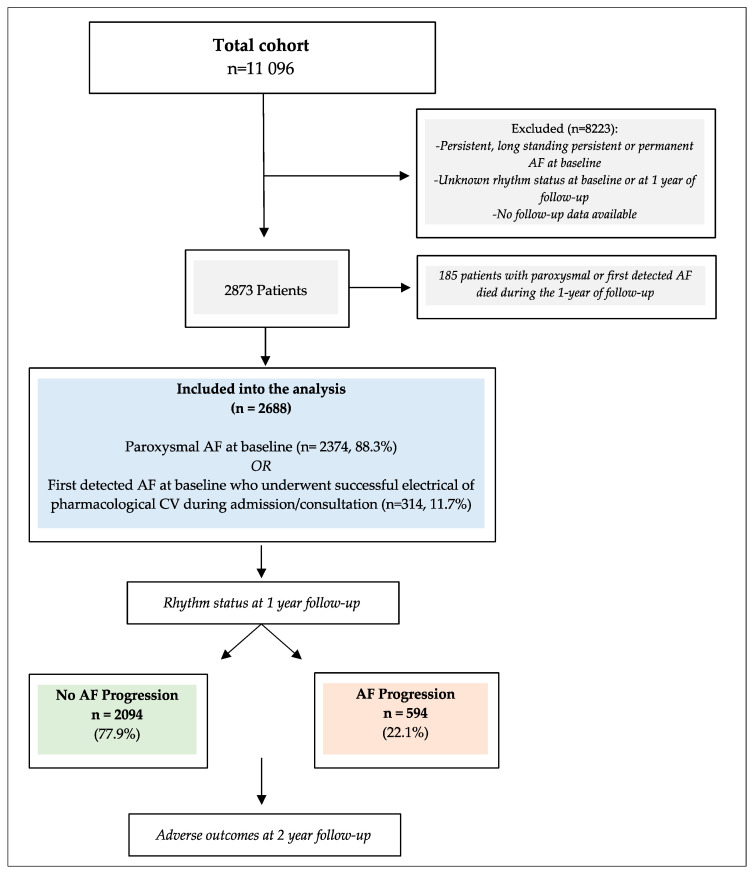
Methods: We analyzed patients enrolled in a prospective cohort study of AF patients. Patients with paroxysmal AF at baseline or first-detected AF (with successful cardioversion) were included. According to rhythm status at 1 year, patients were stratified into: (i) No AF progression and (ii) AF progression. All-cause death was the primary outcome.
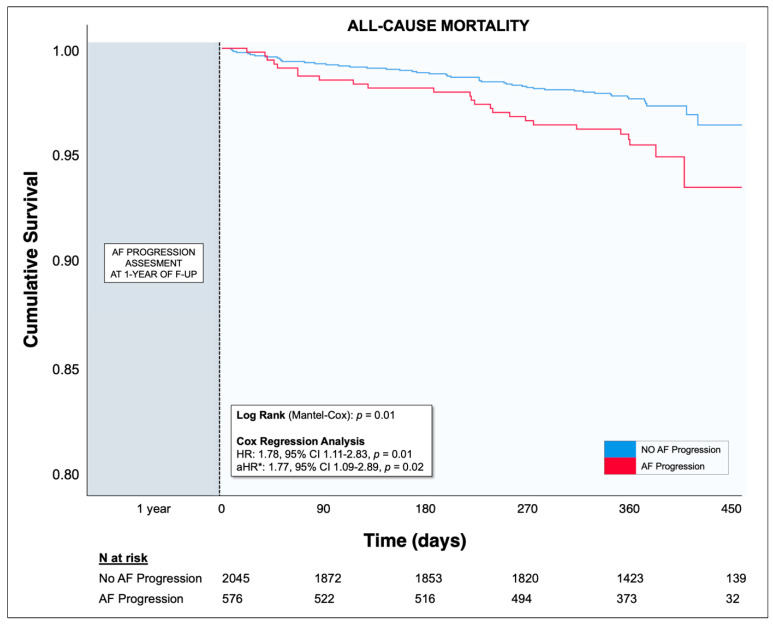
Results: A total of 2688 patients were included (median age 67 years, interquartile range 60-75, females 44.7%). At 1-year of follow-up, 2094 (77.9%) patients showed no AF progression, while 594 (22.1%) developed persistent or permanent AF. On multivariable logistic regression analysis, no physical activity (odds ratio [OR] 1.35, 95% CI 1.02-1.78), valvular heart disease (OR 1.63, 95% CI 1.23-2.15), left atrial diameter (OR 1.03, 95% CI 1.01-1.05), or left ventricular ejection fraction (OR 0.98, 95% CI 0.97-1.00) were independently associated with AF progression at 1 year. After the assessment at 1 year, the patients were followed for an extended follow-up of 371 days, and those with AF progression were independently associated with a higher risk for all-cause death (adjusted hazard ratio 1.77, 95% CI 1.09-2.89) compared to no-AF-progression patients.
Conclusions: In a contemporary cohort of AF patients, a substantial proportion of patients presenting with paroxysmal or first-detected AF showed progression of the AF pattern within 1 year, and clinical factors related to cardiac remodeling were associated with progression. AF progression was associated with an increased risk of all-cause mortality.
Keywords: atrial fibrillation; atrial fibrillation type; death; outcomes; progression; registry; remodeling.
Conflict of interest statement
G.B.: small speaker fee from Bayer, Boston, Boehringer Ingelheim, Brystol Myers Squibb, Janssen and Sanofi. L.F.: consultant or speaker for Bayer, BMS/Pfizer, Boehringer Ingelheim, Medtronic, Novartis, and XO. F.M.: advisor fees Boehringer-Ingelheim; research grants Ferrer; speaker fees Boehringer-Ingelheim, Astra-Zeneca, Pfizer, and Bayer; TP: consultant for Bayer and Pfizer (no fees). G.A.D.: small speaker fees from Boehringer-Ingelheim, Pfizer, Bayer, Sanofi, and Zentiva; G.Y.H.L.: consultant and speaker for Bayer/Janssen, BMS/Pfizer, Boehringer Ingelheim, Anthem, and Daiichi-Sankyo. (No fees were directly received personally.) All the disclosures occurred outside the submitted work. The other authors have no disclosures to declare.
Figures
References
-
- Potpara T.S., Lip G.Y.H., Blomstrom-Lundqvist C., Boriani G., Van Gelder I.C., Heidbuchel H., Hindricks G., Camm A.J. The 4S-AF Scheme (Stroke Risk; Symptoms; Severity of Burden; Substrate): A Novel Approach to In-Depth Characterization (Rather than Classification) of Atrial Fibrillation. Thromb. Haemost. 2020;121:270–278. doi: 10.1055/s-0040-1716408. - DOI - PubMed
-
- Hindricks G., Potpara T., Dagres N., Arbelo E., Bax J.J., Blomström-Lundqvist C., Boriani G., Castella M., Dan G.-A., Dilaveris P.E., et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021;42:373–498. doi: 10.1093/eurheartj/ehaa612. - DOI - PubMed
-
- De With R.R., Marcos E.G., Dudink E.A.M.P., Spronk H.M., Crijns H.J.G.M., Rienstra M., Van Gelder I.C. Atrial fibrillation progression risk factors and associated cardiovascular outcome in well-phenotyped patients: Data from the AF-RISK study. Europace. 2019;22:352–360. doi: 10.1093/europace/euz339. - DOI - PubMed
