

Laboratory Diagnostic of Acute Kidney Injury and Its Progression: Risk of Underdiagnosis in Female and Elderly Patients
- PMID: 36769739
- PMCID: PMC9917506
- DOI: 10.3390/jcm12031092
Laboratory Diagnostic of Acute Kidney Injury and Its Progression: Risk of Underdiagnosis in Female and Elderly Patients
Abstract
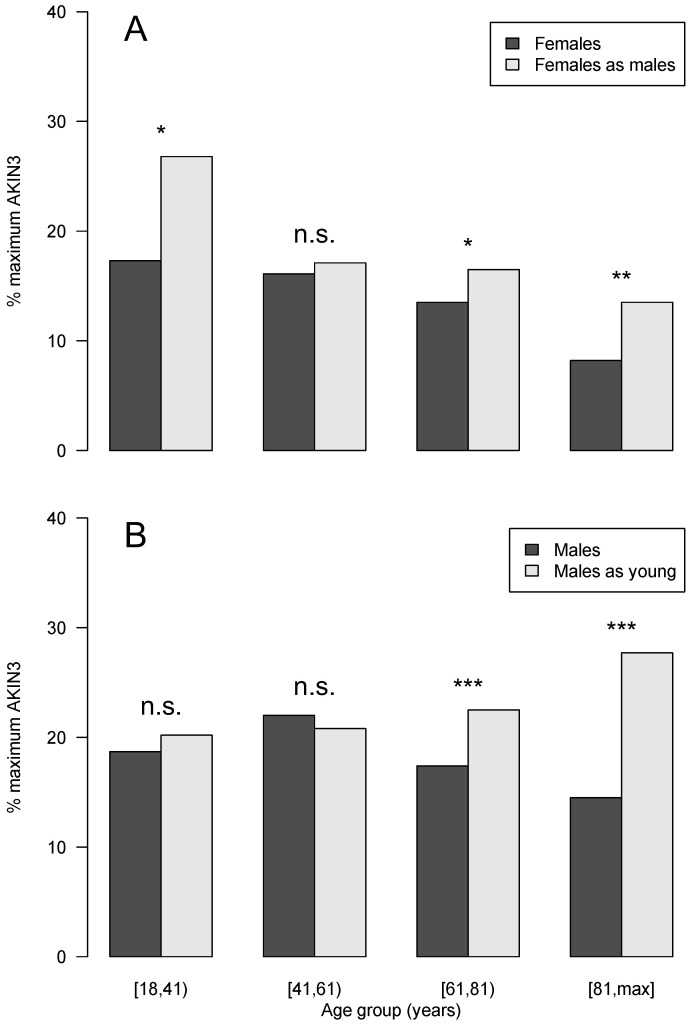
Acute kidney injury (AKI) is a common disease, with high morbidity and mortality rates. In this study, we investigated the potential influence of sex and age on laboratory diagnostics and outcomes. It is known that serum creatinine (SCr) has limitations as a laboratory diagnostic parameter for AKI due to its dependence on muscle mass, which may lead to an incorrect or delayed diagnosis for certain patient groups, such as women and the elderly. Overall, 7592 cases with AKI, hospitalized at the University of Leipzig Medical Center (ULMC) between 1st January 2017 and 31st December 2019, were retrospectively analyzed. The diagnosis and staging of AKI were performed according to the Kidney Disease: Improving Global Outcomes (KDIGO) guidelines, based on the level and dynamics of SCr. The impact of sex and age was analyzed by the recalculation of a female to male and an old to young SCr using the CKD-EPI equation. In our study cohort progressive AKI occurred in 19.2% of all cases (n = 1458). Female cases with AKI were underrepresented (40.4%), with a significantly lower first (-3.5 mL/min) and last eGFR (-2.7 mL/min) (p < 0.001). The highest incidence proportion of AKI was found in the [61-81) age group in female (49.5%) and male (52.7%) cases. Females with progressive AKI were underrepresented (p = 0.04). By defining and staging AKI on the basis of relative and absolute changes in the SCr level, it is more difficult for patients with low muscle mass and, thus, a lower baseline SCr to be diagnosed by an absolute SCr increase. AKIN1 and AKIN3 can be diagnosed by a relative or absolute change in SCr. In females, both stages were less frequently detected by an absolute criterion alone (AKIN1 ♀ 20.2%, ♂ 29.5%, p < 0.001; AKIN3 ♀ 13.4%, ♂ 15.2%, p < 0.001). A recalculated SCr for females (as males) and males (as young males) displayed the expected increase in AKI occurrence and severity with age and, in general, in females. Our study illustrates how SCr, as the sole parameter for the diagnosis and staging of AKI, bears the risk of underdiagnosis of patient groups with low muscle mass, such as women and the elderly. A sex- and age-adapted approach might offer advantages.
Keywords: CDSS; KDIGO; acute kidney injury; age and sex; elderly; laboratory diagnostics; serum creatinine; women.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Khadzhynov D., Schmidt D., Hardt J., Rauch G., Gocke P., Eckardt K.-U., Schmidt-Ott K.M. The Incidence of Acute Kidney Injury and Associated Hospital Mortality: A Retrospective Cohort Study of Over 100 000 Patients at Berlin‘s Charité Hospital. Dtsch. Ärzteblatt Int. 2019;116:397. doi: 10.3238/arztebl.2019.0397. - DOI - PMC - PubMed
-
- Kister T.S., Remmler J., Schmidt M., Federbusch M., Eckelt F., Isermann B., Richter H., Wehner M., Krause U., Halbritter J., et al. Acute kidney injury and its progression in hospitalized patients—Results from a retrospective multicentre cohort study with a digital decision support system. PLoS ONE. 2021;16:e0254608. doi: 10.1371/journal.pone.0254608. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
