

Electric Cardioversion vs. Pharmacological with or without Electric Cardioversion for Stable New-Onset Atrial Fibrillation: A Systematic Review and Meta-Analysis
- PMID: 36769812
- PMCID: PMC9918032
- DOI: 10.3390/jcm12031165
Electric Cardioversion vs. Pharmacological with or without Electric Cardioversion for Stable New-Onset Atrial Fibrillation: A Systematic Review and Meta-Analysis
Abstract
Background: There is no clear consensus on the preference for pharmacological cardioversion (PC) in comparison to electric cardioversion (EC) for hemodynamically stable new-onset atrial fibrillation (NOAF) patients presenting to the emergency department (ED).
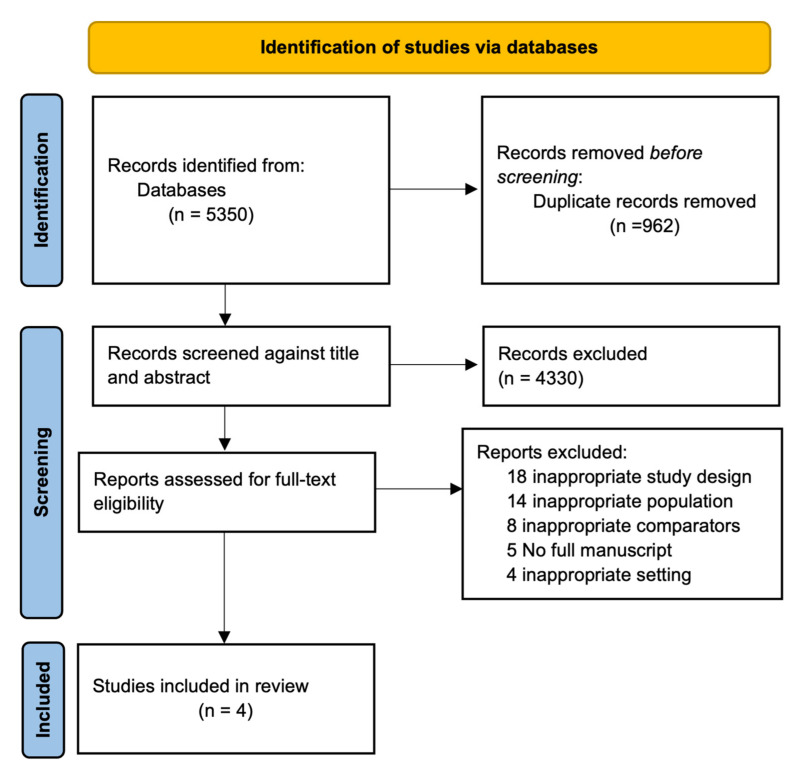
Methods: A systematic review and meta-analysis was conducted to assess PC (whether being followed by EC or not) vs. EC in achieving cardioversion for hemodynamically stable NOAF patients. PubMed, PubMed Central, Embase, Scopus, and Cochrane databases were searched to include relevant studies until 7 March 2022. The primary outcome was the successful restoration of sinus rhythm, and secondary outcomes included emergency department (ED) revisits with atrial fibrillation (AF), hospital readmission rate, length of hospital stay, and cardioversion-associated adverse events.
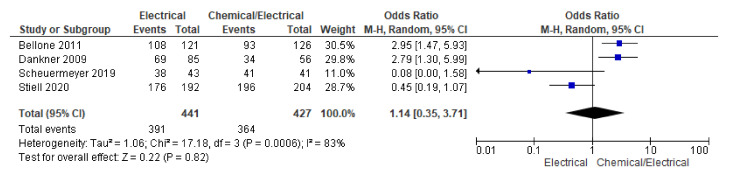
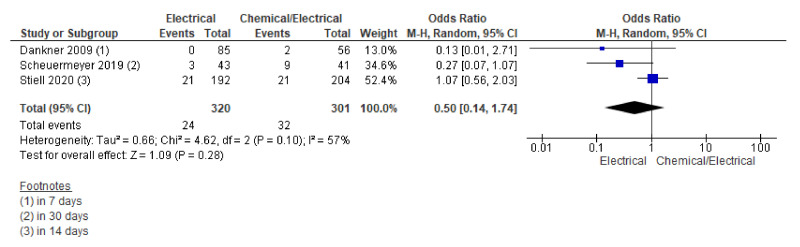
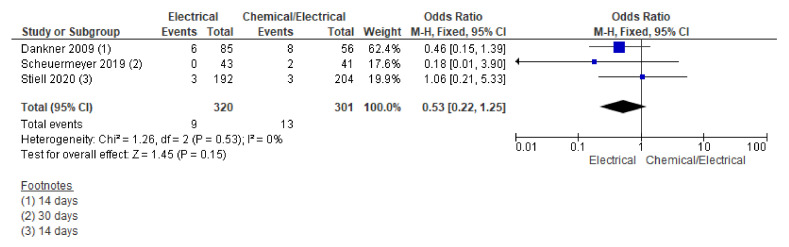
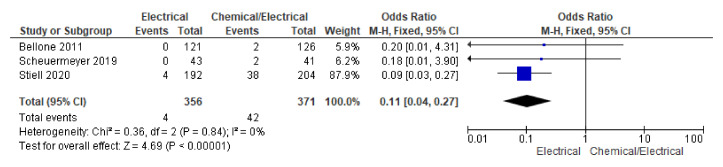
Results: A total of three randomized controlled trials (RCTs) and one observational study were included. There was no difference in the rates of successful restoration to sinus rhythm (88.66% vs. 85.25%; OR 1.14, 95% CI 0.35-3.71; n = 868). There was no statistical difference across the two groups for ED revisits with AF, readmission rates, length of hospital stay, and cardioversion-associated adverse effects, with the exception of hypotension, whose incidence was lower in the EC group (OR 0.11, 95% CI 0.04-0.27: n = 727).
Conclusion: This meta-analysis suggests that there is no difference in successful restoration of sinus rhythm with either modality among patients with hemodynamically stable NOAF.
Keywords: cardioversion; electrical cardioversion; new-onset atrial fibrillation; pharmacological cardioversion.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Hindricks G., Potpara T., Dagres N., Bax J.J., Boriani G., Dan G.A., Fauchier L., Kalman J.M., Lane D.A., Lettino M., et al. 2020 ESC Guidelines for the Diagnosis and Management of Atrial Fibrillation Developed in Collaboration with the European Association for Cardio-Thoracic Surgery (EACTS) Eur. Heart J. 2021;42:373–498. - PubMed
-
- Stiell I.G., Sivilotti M.L.A., Taljaard M., Birnie D., Vadeboncoeur A., Hohl C.M., Mcrae A.D., Rowe B.H., Brison R.J., Thiruganasambandamoorthy V., et al. Electrical versus Pharmacological Cardioversion for Emergency Department Patients with Acute Atrial Fibrillation (RAFF2): A Partial Factorial Randomised Trial. Lancet. 2020;395:339–349. doi: 10.1016/S0140-6736(19)32994-0. - DOI - PubMed
-
- Dankner R., Shahar A., Novikov I., Agmon U., Ziv A., Hod H. Treatment of Stable Atrial Fibrillation in the Emergency Department: A Population-Based Comparison of Electrical Direct-Current versus Pharmacological Cardioversion or Conservative Management. Cardiology. 2009;112:270–278. doi: 10.1159/000151703. - DOI - PubMed
-
- PROSPERO. [(accessed on 26 December 2022)]. Available online: https://www.crd.york.ac.uk/prospero/#recordDetails.
Publication types
LinkOut - more resources
Full Text Sources
