

Dietary Exposures and Interventions in Inflammatory Bowel Disease: Current Evidence and Emerging Concepts
- PMID: 36771288
- PMCID: PMC9921630
- DOI: 10.3390/nu15030579
Dietary Exposures and Interventions in Inflammatory Bowel Disease: Current Evidence and Emerging Concepts
Abstract
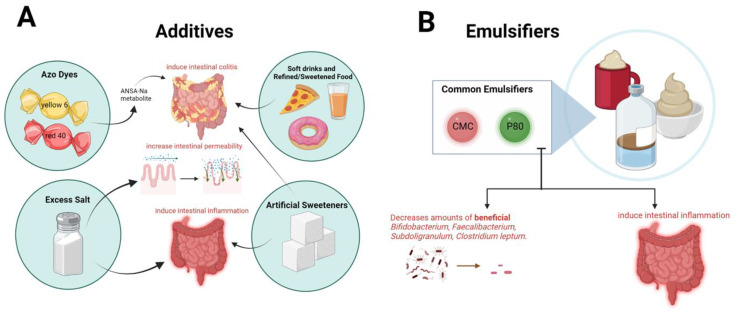
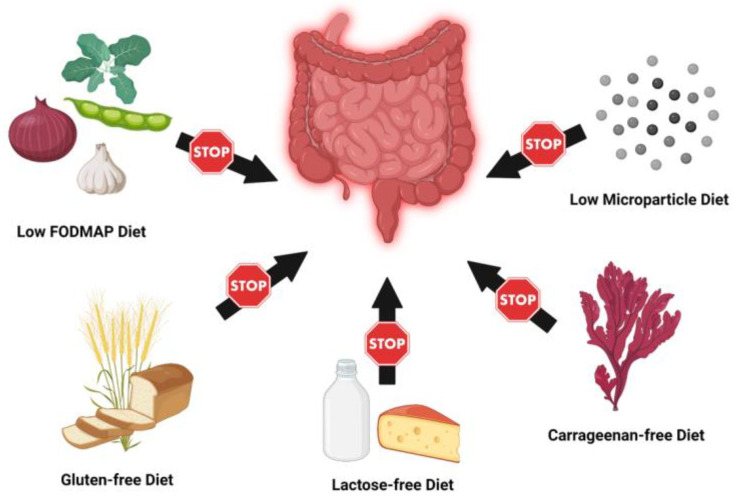
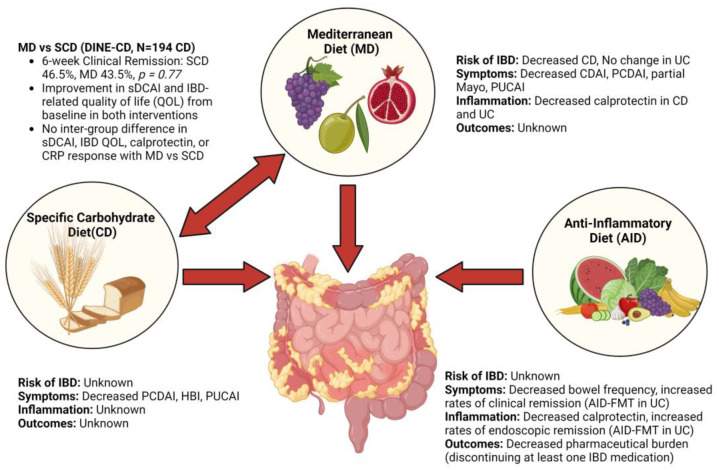
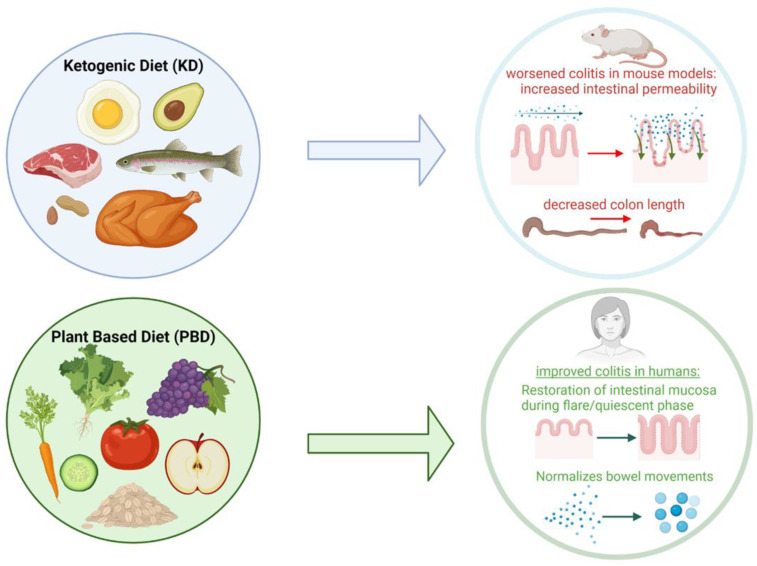
Diet is intimately linked to the gastrointestinal (GI) tract and has potent effects on intestinal immune homeostasis. Inflammatory bowel disease (IBD) is characterized by chronic inflammation of the GI tract. The therapeutic implications of diet in patients with IBD have received significant attention in recent years. In this review, we provide a contemporary and comprehensive overview of dietary exposures and interventions in IBD. Epidemiological studies suggest that ultra-processed foods, food additives, and emulsifiers are associated with a higher incidence of IBD. Exclusion and elimination diets are associated with improved symptoms in patients with IBD, but no effects on objective markers of inflammation. Specific dietary interventions (e.g., Mediterranean, specific carbohydrate, high fiber, ketogenic, anti-inflammatory diets) have been shown to reduce symptoms, improve inflammatory biomarkers, and quality of life metrics to varying degrees, but these studies are limited by study design, underpowering, heterogeneity, and confounding. To date, there is no robust evidence that any dietary intervention alone may replace standard therapies in patients with IBD. However, diet may play an adjunct role to induce or maintain clinical remission with standard IBD therapies. The results of novel dietary trials in IBD such as personalized fiber, intermittent fasting, and time-restricted diets are eagerly awaited.
Keywords: Crohn’s disease; clinical trials; diet; epidemiology; food; inflammatory bowel disease; ulcerative colitis.
Conflict of interest statement
Authors have no conflict of interests or financial disclosures relevant to this manuscript.
Figures
References
-
- Teo K., Chow C.K., Vaz M., Rangarajan S., Yusuf S. PURE Investigators-Writing Group. The Prospective Urban Rural Epidemiology (PURE) study: Examining the impact of societal influences on chronic noncommunicable diseases in low-, middle-, and high-income countries. Am. Heart J. 2009;158:1–7.e1. doi: 10.1016/j.ahj.2009.04.019. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
