

Chronic disease clusters are associated with prolonged, bothersome, and multisite musculoskeletal pain: a population-based study on Northern Finns
- PMID: 36773018
- PMCID: PMC9930817
- DOI: 10.1080/07853890.2023.2177723
Chronic disease clusters are associated with prolonged, bothersome, and multisite musculoskeletal pain: a population-based study on Northern Finns
Abstract
Background: Chronic diseases often accumulate with musculoskeletal (MSK) pain. However, less evidence is available on idiosyncratic patterns of chronic diseases and their relationships with the severity of MSK pain in general MSK pain populations.
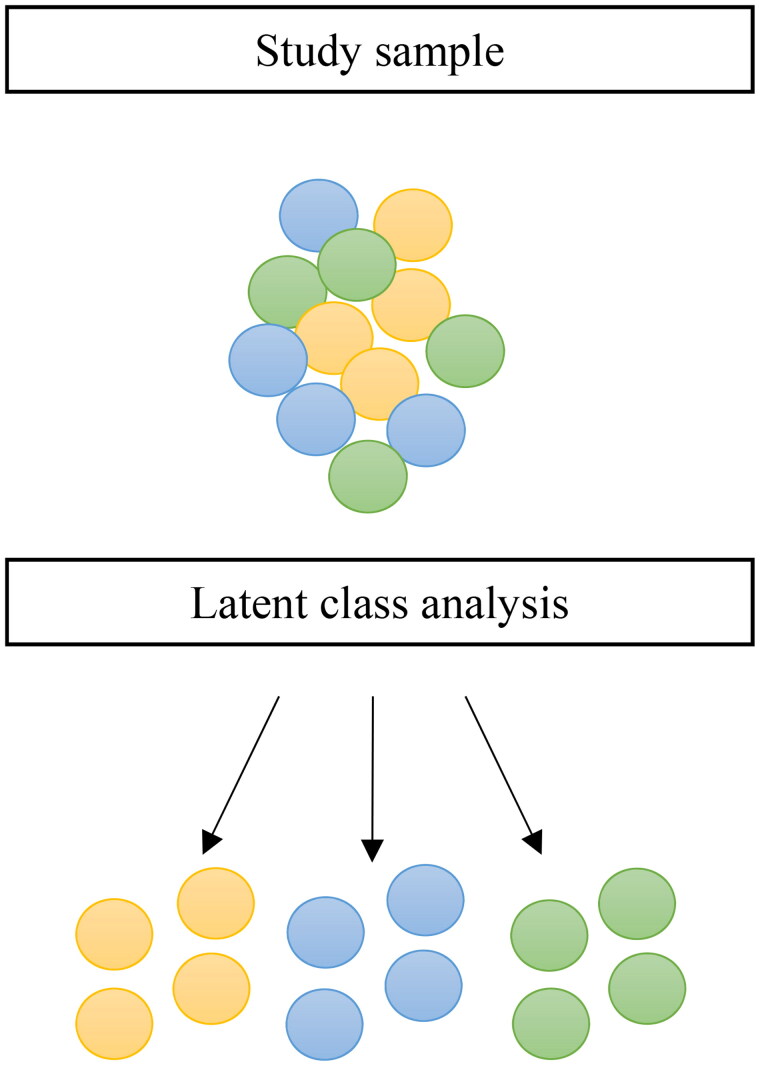
Material and methods: Questionnaire-based data on physician-diagnosed chronic diseases, MSK pain and its dimensions (frequency, intensity, bothersomeness, and the number of pain sites), and confounders were collected from the Northern Finland Birth Cohort 1966 at the age of 46. Latent Class Analysis (LCA) was used to identify chronic disease clusters among individuals who reported any MSK pain within the previous year (n = 6105). The associations between chronic disease clusters, pain dimensions, and severe MSK pain, which was defined as prolonged (over 30 d within the preceding year), bothersome (Numerical Rating Scale >5), and multisite (two or more pain sites) pain, were analyzed using logistic regression and general linear regression models, adjusted for sex and educational level (n for the full sample = 4768).
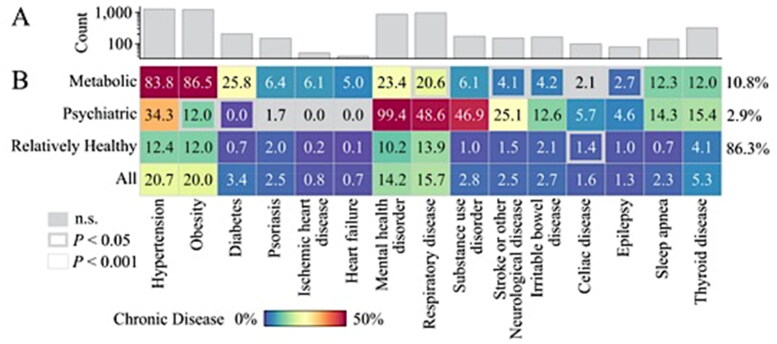
Results: LCA resulted in three clusters: Metabolic (10.8% of the full sample), Psychiatric (2.9%), and Relatively Healthy (86.3%). Compared to the Relatively Healthy cluster, the Metabolic and Psychiatric clusters had higher odds for daily pain and higher mean pain intensity, bothersomeness, and the number of pain sites. Similarly, the odds for severe MSK pain were up to 75% (95% confidence interval: 44%-113%) and 155% (81%-259%) higher in the Metabolic and Psychiatric clusters, respectively, after adjustments for sex and educational level.
Conclusions: Distinct patterns of chronic disease accumulation can be identified in the general MSK pain population. It seems that mental and metabolic health are at interplay with severe MSK pain. These findings suggest a potential need to screen for psychiatric and metabolic entities of health when treating working-aged people with MSK pain.Key messagesThis large study on middle-aged people with musculoskeletal pain aimed to examine the idiosyncratic patterns of chronic diseases and their relationships with the severity of musculoskeletal pain. Latent class cluster analysis identified three chronic disease clusters: Psychiatric, Metabolic, and Relatively Healthy. People with accumulated mental (Psychiatric cluster) or metabolic diseases (Metabolic cluster) experienced more severe pain than people who were relatively healthy (Relatively Healthy cluster). These findings suggest a potential need to screen for psychiatric and metabolic entities of health when treating working-aged people with MSK pain.
Keywords: Musculoskeletal pain; chronic diseases; cohort study; pain severity.
Conflict of interest statement
No potential conflict of interest was reported by the author(s).
Figures
References
-
- Duffield SJ, Ellis BM, Goodson N, et al. The contribution of musculoskeletal disorders in multimorbidity: implications for practice and policy. Best Pract Res Clin Rheumatol. 2017;31(2):129–144. - PubMed
-
- van der Zee-Neuen A, Putrik P, Ramiro S, et al. Impact of chronic diseases and multimorbidity on health and health care costs: the additional role of musculoskeletal disorders. Arthritis Care Res. 2016;68(12):1823–1831. - PubMed
-
- Lowe D, Taylor M, Hill S.. Changing definitions altered multimorbidity prevalence, but not burden associations, in a musculoskeletal population. J Clin Epidemiol. 2016;78:116–126. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials