

Alveolar capillary dysplasia with misalignment of pulmonary veins in a premature newborn: the role of lung ultrasound
- PMID: 36774442
- PMCID: PMC9922097
- DOI: 10.1186/s13089-023-00310-z
Alveolar capillary dysplasia with misalignment of pulmonary veins in a premature newborn: the role of lung ultrasound
Abstract
Background: Alveolar capillary dysplasia with misalignment of pulmonary veins (ACD/MPV) is a lethal neonatal lung disorder characterized by the decrease of the alveolar units, abnormalities in the air-blood barrier of the lung, and impaired gas exchange. Typically, it affects a full-term newborn; the symptoms usually start within a few hours after birth, resulting in severe respiratory distress and pulmonary hypertension. In most of the cases, this disorder is refractory to conventional pulmonary support.
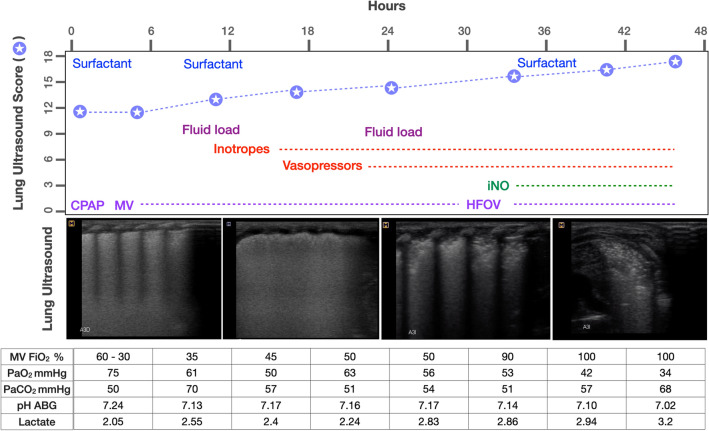
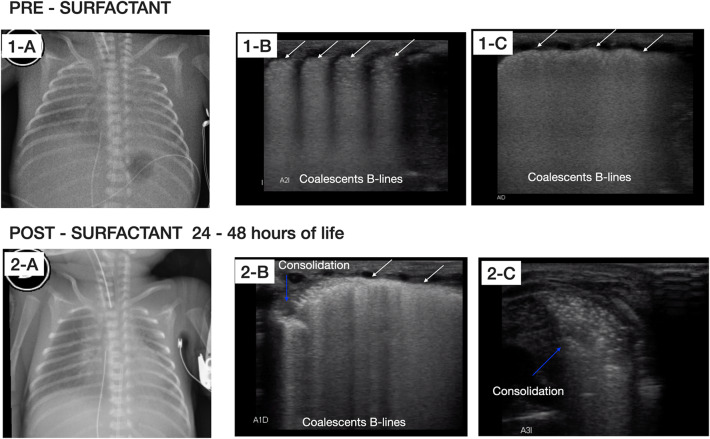
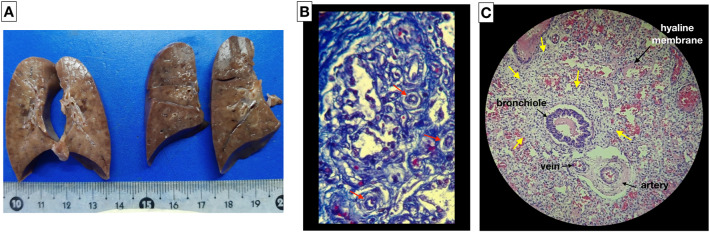
Case presentation: We report a case of a newborn male of 29 weeks gestational age, with birth weight of 850 g and intrauterine growth restriction. Severe respiratory distress appeared a few minutes after birth; non-invasive ventilatory support was provided in the delivery room and, as a consequence of persistent respiratory failure, he was admitted to the neonatal intensive care unit (NICU) where mechanical ventilation was required. Due to the symptoms and pulmonary ultrasound pattern suggestive of respiratory distress syndrome, surfactant treatment was administered. Lung ultrasound (LU) was used for monitoring the responsiveness to surfactant; severe pulmonary hypertension ensued, followed by respiratory failure, refractory shock, and death within 48 h. Owing to the poor response to the established therapy, ACD/MPV was suspected. The diagnosis was confirmed through autopsy. The main goal of this case report is to show the role of LU for monitoring the evolution of this disorder.
Conclusion: LU could provide essential information to help diagnose and follow-up the underlying cause of persistent pulmonary hypertension of the newborn in an earlier and more effective way than chest X-ray. LU is suitable for routine monitoring of lung disease in the NICU.
Keywords: Congenital alveolar dysplasia; Lung ultrasound; Neonate; Pulmonary hypertension; Respiratory distress.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous