

Increasing Pancreatic Cancer Incidence in Young Women in the United States: A Population-Based Time-Trend Analysis, 2001-2018
- PMID: 36775072
- PMCID: PMC11364483
- DOI: 10.1053/j.gastro.2023.01.022
Increasing Pancreatic Cancer Incidence in Young Women in the United States: A Population-Based Time-Trend Analysis, 2001-2018
Abstract
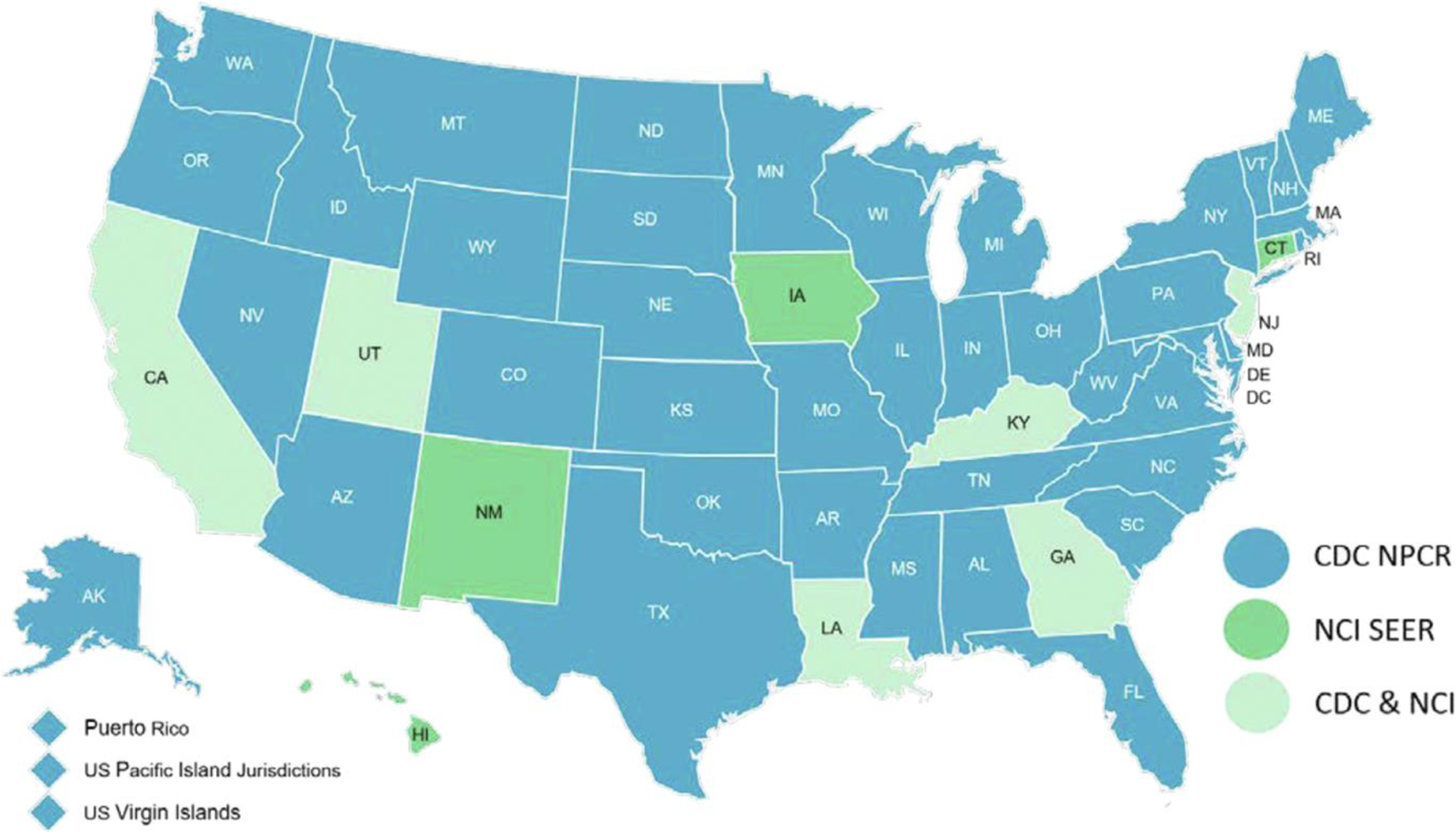
Background & aims: Previous studies have shown an increasing incidence of pancreatic cancer (PC), especially in younger women; however, this has not been externally validated. In addition, there are limited data about contributing factors to this trend. We report age and sex-specific time-trend analysis of PC age-adjusted incidence rates (aIRs) using the National Program of Cancer Registries database without Surveillance Epidemiology and End Results data.
Methods: PC aIR, mortality rates, annual percentage change, and average annual percentage change (AAPC) were calculated and assessed for parallelism and identicalness. Age-specific analyses were conducted in older (≥55 years) and younger (<55 years) adults. PC incidence based on demographics, tumor characteristics, and mortality were evaluated in younger adults.
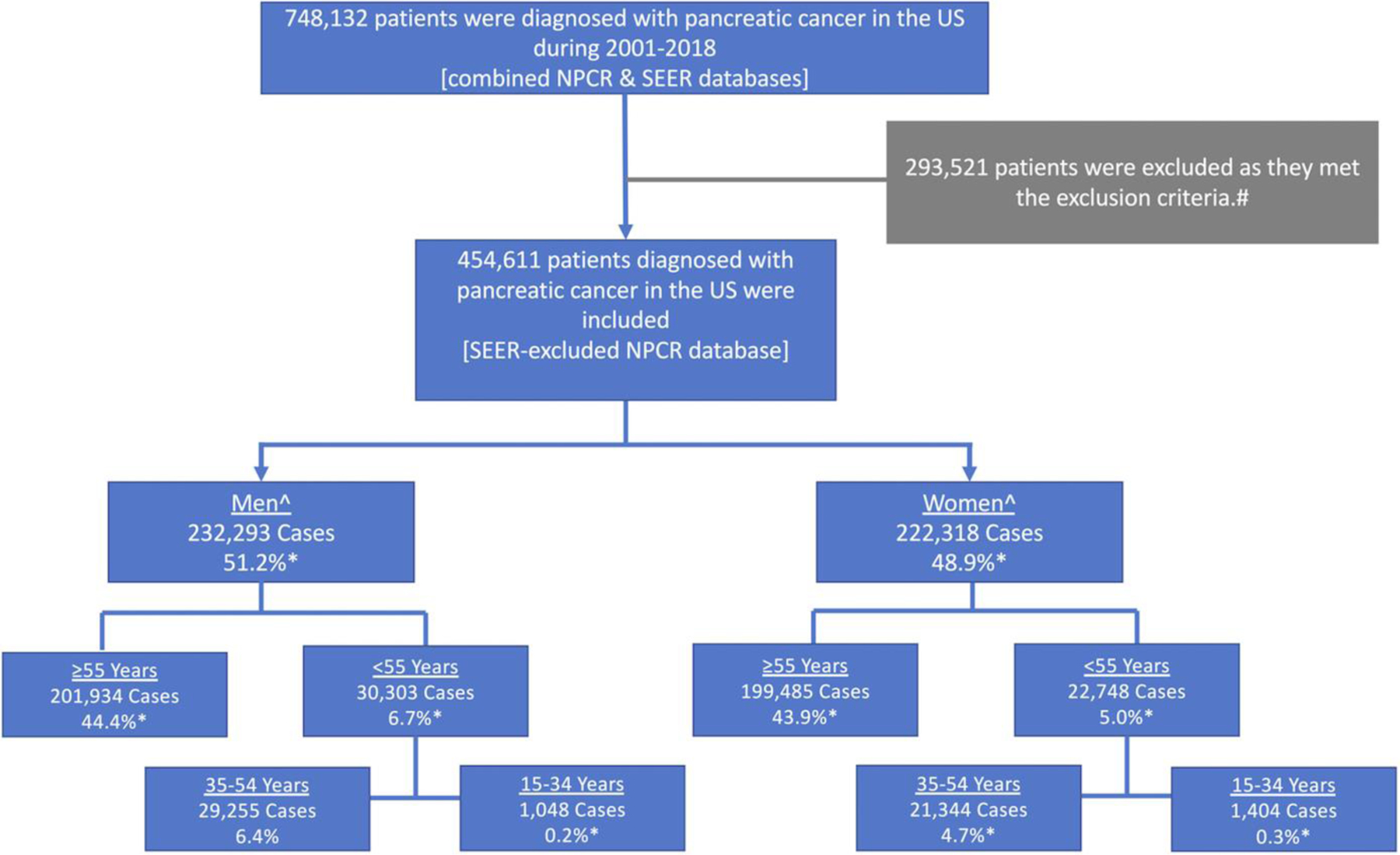
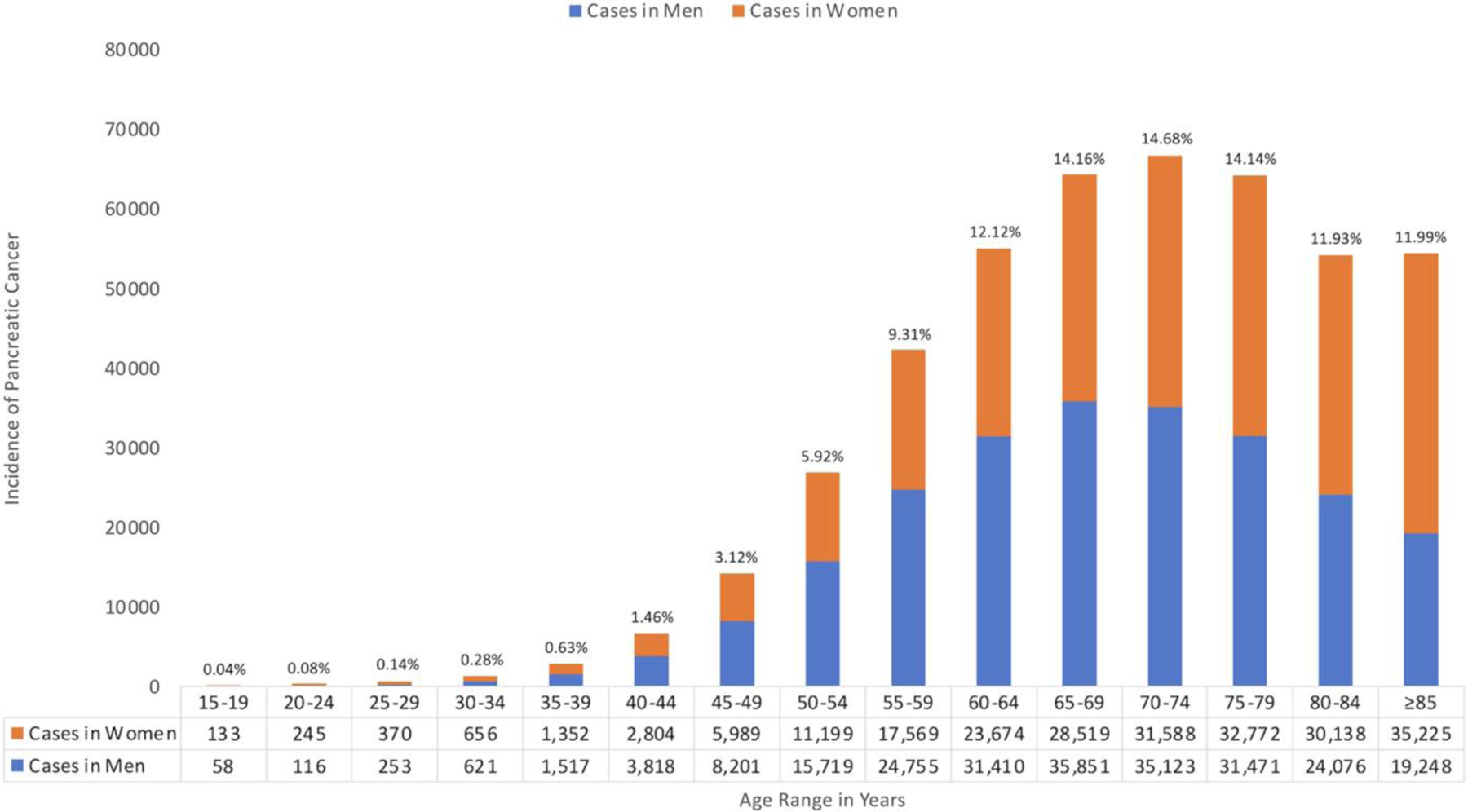
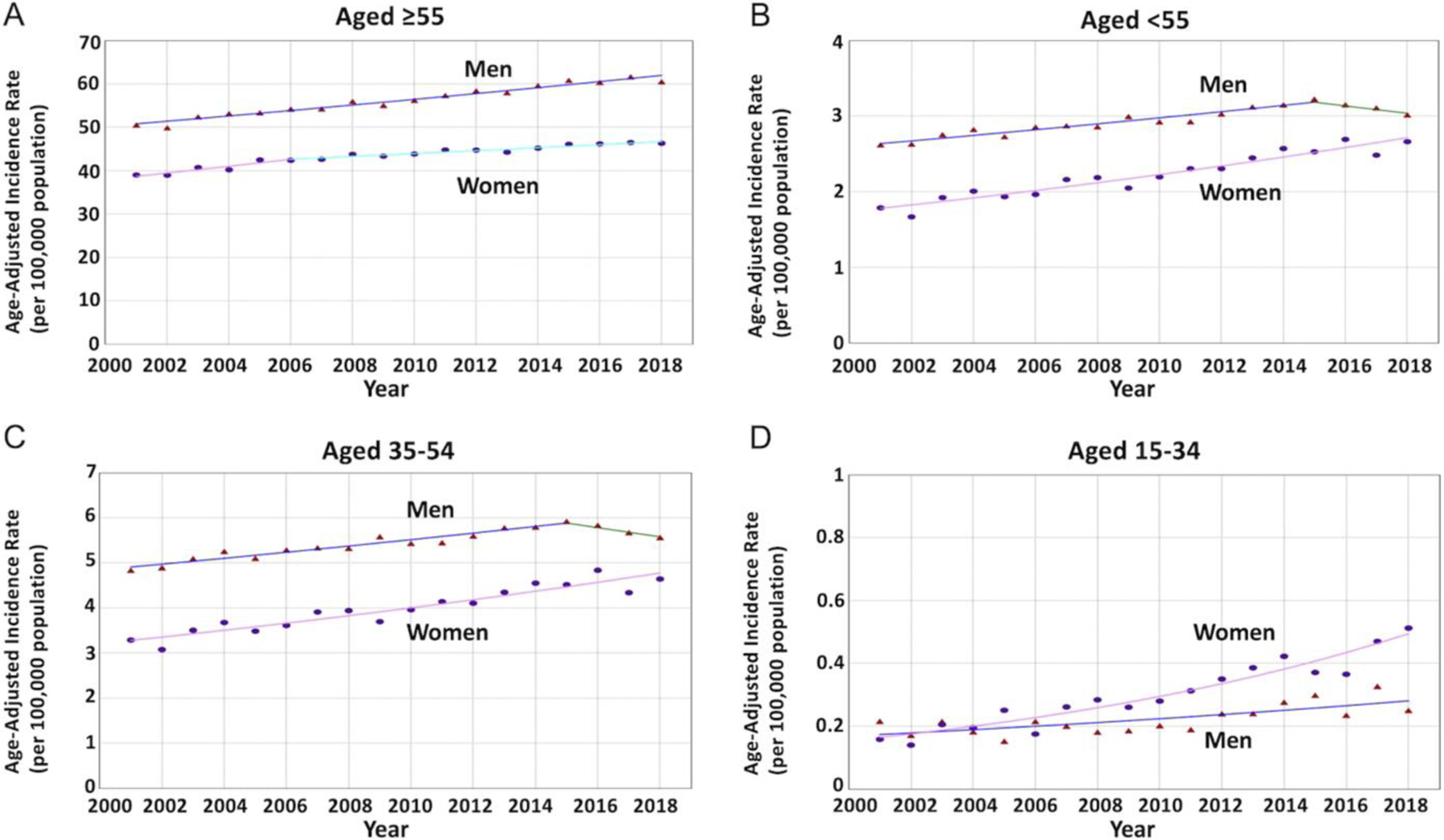
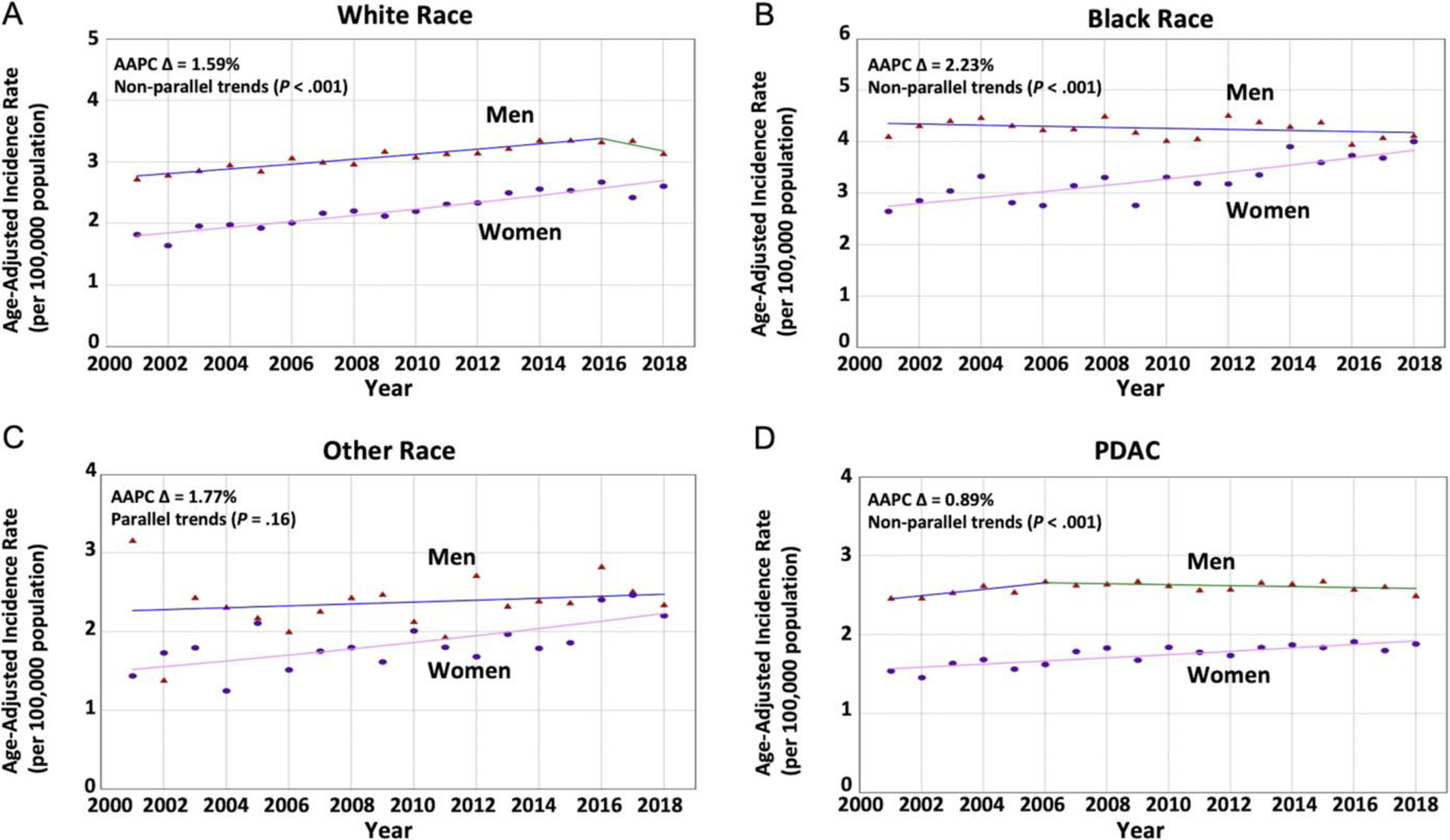
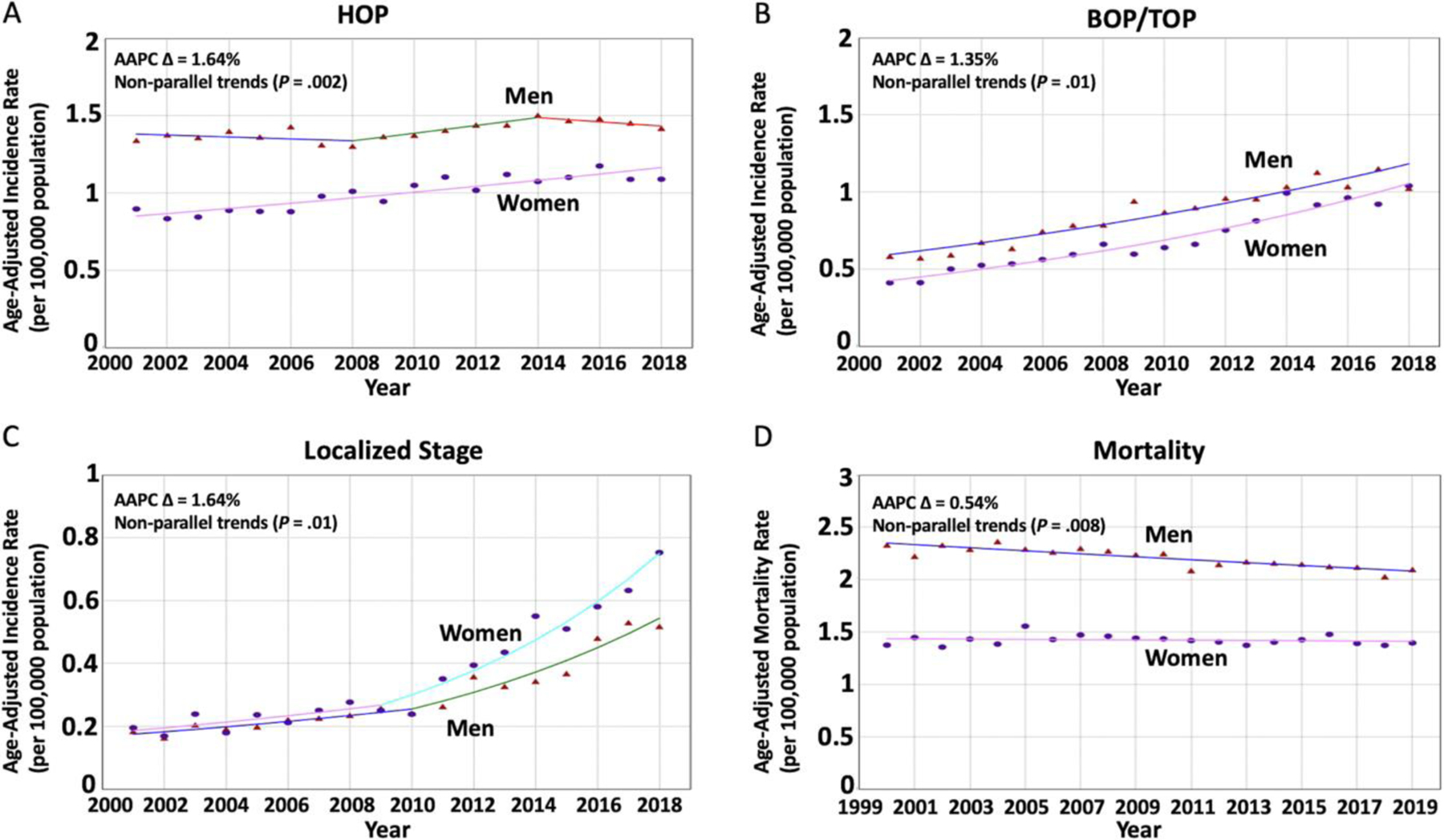
Results: A total of 454,611 patients were diagnosed with PC between 2001 and 2018 with significantly increasing aIR in women (AAPC = 1.27%) and men (AAPC = 1.14%) without a difference (P = .37). Similar results were seen in older adults. However, in younger adults (53,051 cases; 42.9% women), women experienced a greater increase in aIR than men (AAPCs = 2.36%, P < .001 vs 0.62%, P = 0.62) with nonparallel trends (P < .001) and AAPC difference of 1.74% (P < .001). This AAPC difference appears to be due to rising aIR in Blacks (2.23%; P < .001), adenocarcinoma histopathologic subtype (0.89%; P = .003), and location in the head-of-pancreas (1.64%; P < .001). PC mortality was found to be unchanged in women but decreasing in counterpart men (AAPC difference = 0.54%; P = .001).
Conclusion: Using nationwide data, covering ≈64.5% of the U.S. population, we externally validate a rapidly increasing aIR of PC in younger women. There was a big separation of the incidence trend between women and men aged 15-34 years between 2001 and 2018 (>200% difference), and it did not show slowing down.
Keywords: Epidemiology; Incidence; Mortality; Pancreatic Cancer; Sex.
Copyright © 2023 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of interest
The authors disclose no conflicts.
Figures
Comment in
-
Cannabis Could Be the Missing Environmental Carcinogen Hiding in Plain View.Gastroenterology. 2023 Oct;165(4):1092-1093. doi: 10.1053/j.gastro.2023.02.050. Epub 2023 Apr 11. Gastroenterology. 2023. PMID: 37054753 No abstract available.
References
-
- NIH National Cancer Institute SEER Program. Cancer Stat Facts: Pancreatic Cancer. Available at: https://seer.cancer.gov/statfacts/html/pancreas.html. Accessed November 6, 2022.
-
- Siegel RL, Miller KD, Fuchs HE, et al. Cancer Statistics, 2021. CA Cancer J Clin 2021;71:7–33. - PubMed
-
- U.S. Cancer Statistics Working Group. U.S. Cancer Statistics. Data Visualizations Tool, based on 2021 submission data (1999–2019): U.S. Department of Health and Human Services, Centers for Disease Control and Prevention and National Cancer Institute. Available at: https://www.cdc.gov/cancer/dataviz. Released November 2022. Accessed November 9, 2022.
-
- Bauer MR, Bright EE, MacDonald JJ, et al. Quality of life in patients with pancreatic cancer and their caregivers: a systematic review. Pancreas 2018;47:368–375. - PubMed
