

Carotid Intima Media Thickness and Risk Factor for Atherosclerosis: Tohoku Medical Megabank Community-Based Cohort Study
- PMID: 36775331
- PMCID: PMC10564640
- DOI: 10.5551/jat.64039
Carotid Intima Media Thickness and Risk Factor for Atherosclerosis: Tohoku Medical Megabank Community-Based Cohort Study
Abstract
Aim: We examined the association between the carotid intima medica thickness (cIMT) and risk factors for atherosclerosis based on the Japan Atherosclerosis Society 2022 Atherosclerosis Prevention Guideline.
Methods: Using data from the Tohoku Medical Megabank Community-based Cohort Study, we performed a cross-sectional study that enrolled 13,366 participants (age ≥ 20 years) with an analysis of covariance to assess associations between cIMT and risk factors for atherosclerosis. The maximum common carotid artery was measured using high-resolution B-mode ultrasound. Analysis was conducted in the model adjusted for age, sex, smoking status, drinking status, body mass index (BMI), systolic blood pressure (SBP), glycated hemoglobin (HbA1c), high-density lipoprotein-cholesterol (HDL-C), non-high-density lipoprotein-cholesterol (non-HDL-C), and height.
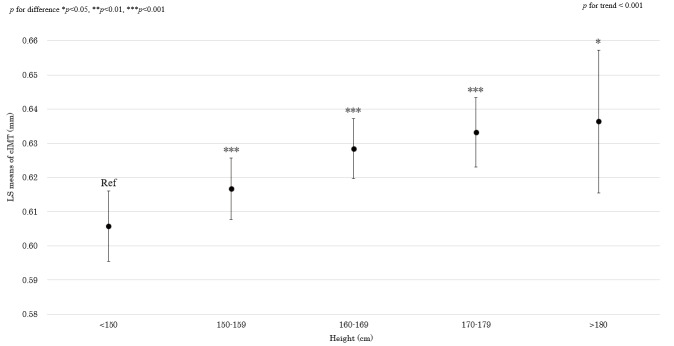
Results: In this study cohort, the average age and cIMT were 57.3 (13.8) years and 0.61 (0.13) mm, respectively, which included 3,988 males (29.8%). Males had a higher cIMT than did the females. Age, height, BMI, SBP, HbA1c, and non-HDL-C were positively associated with cIMT. HDL-C was inversely associated with cIMT. Compared with never drinkers, current drinkers (≥ 46.0 g/day) had a significantly decreased cIMT.
Conclusions: The cIMT was associated with atherosclerosis risk factors including age, sex, BMI, SBP, HbA1c, non-HDL-C, and HDL-C, and adequate control of risks in high-risk individuals might be required to prevent atherosclerotic cardiovascular diseases.
Keywords: Atherosclerosis; Carotid intima media thickness; Epidemiology; Risk factor.
Conflict of interest statement
There are no conflicts of interest.
Figures




References
-
- Japan Atherosclerosis Society (JAS) Guidelines for Prevention of Atherosclerotic Cardiovascular Diseases 2022. Accessed November 24,2022. https: //www.j-athero.org/jp/wp-content/uploads/publications/pdf/GL2022_s/jas_gl2... - PMC - PubMed
-
- O’Leary DH, Polak JF, Kronmal RA, Manolio TA, Burke GL, and Wolfson SK: Carotid-artery intima and media thickness as a risk factor for myocardial infarction and stroke in older adults. Cardiovascular Health Study Collaborative Research Group. N Engl J Med, 1999; 340: 14-22 - PubMed
-
- Nezu T, Hosomi N, Aoki S, and Matsumoto M: Carotid intima-media thickness for atherosclerosis. J Atheroscler Thromb, 2016; 23: 18-31 - PubMed
-
- Mannami T, Konishi M, Baba S, Nishi N, Terao A: Prevalence of asymptomatic carotid atherosclerotic lesions detected by high-resolution ultrasonography and its relation to cardiovascular risk factors in the general population of a Japanese city: the Suita study. Stroke, 1997; 28: 518-525 - PubMed
-
- van der Meer IM, Iglesias del Sol A, Hak AE, Bots ML, Hofman A, and Witteman JC: Risk factors for progression of atherosclerosis measured at multiple sites in the arterial tree: the Rotterdam Study. Stroke, 2003; 34: 2374-2379 - PubMed