

Biomechanical Comparison of Synthetic Polytetrafluoroethylene (PTFE) vs Human Dermal Allograft (HDA), 2 vs 3 Glenoid Anchors, and Suture vs Minitape in Superior Capsule Reconstruction
- PMID: 36776506
- PMCID: PMC9837406
- DOI: 10.1177/15563316221114135
Biomechanical Comparison of Synthetic Polytetrafluoroethylene (PTFE) vs Human Dermal Allograft (HDA), 2 vs 3 Glenoid Anchors, and Suture vs Minitape in Superior Capsule Reconstruction
Abstract
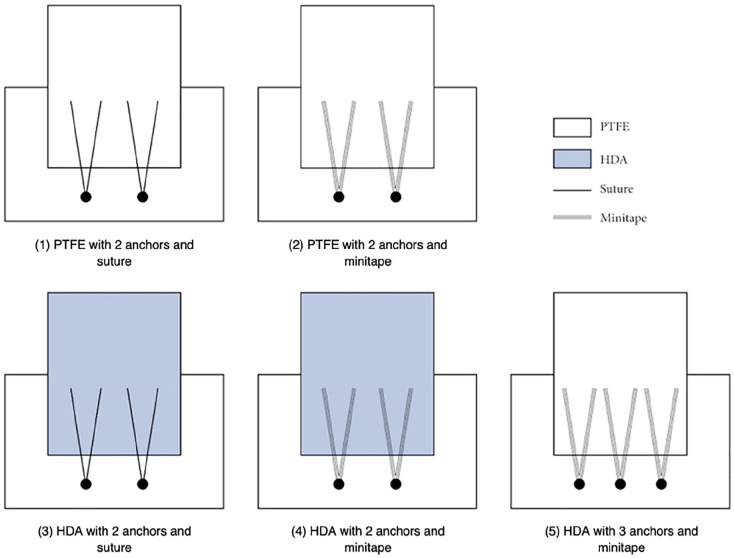
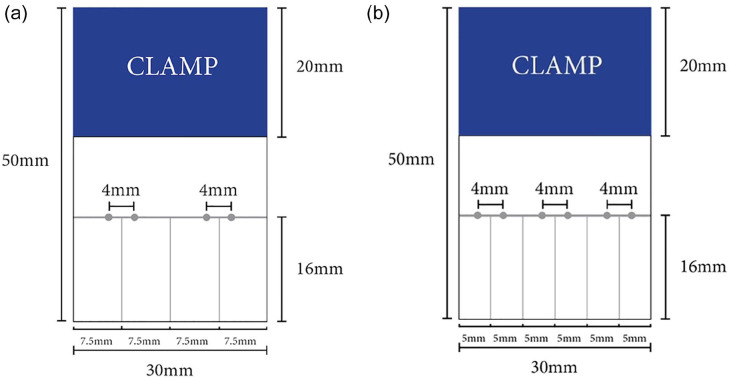
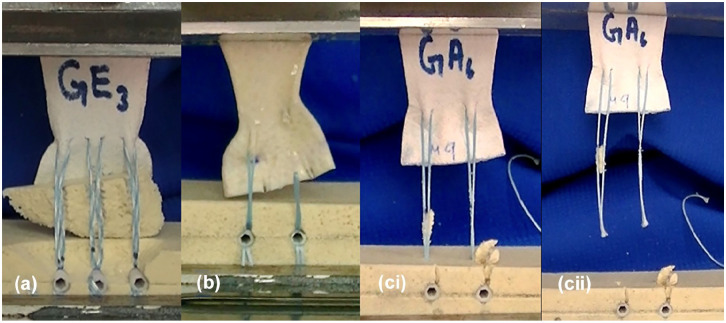
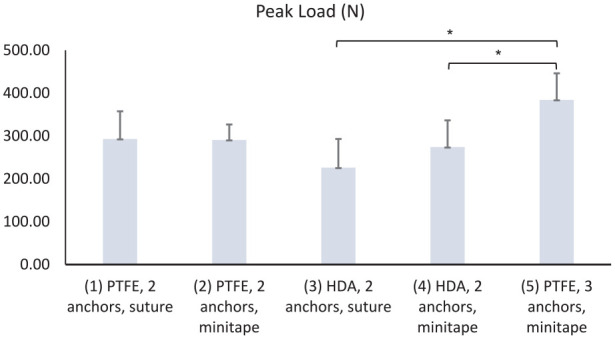
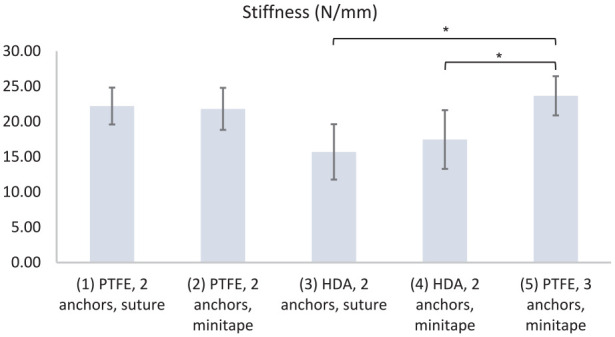
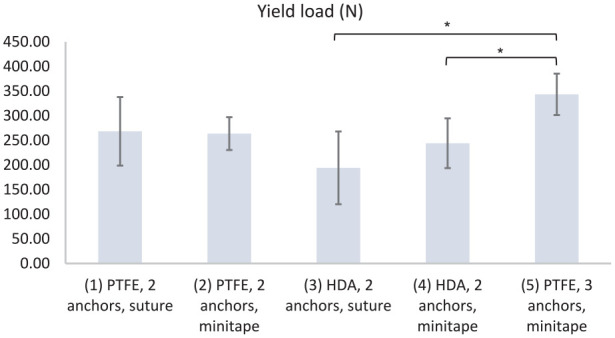
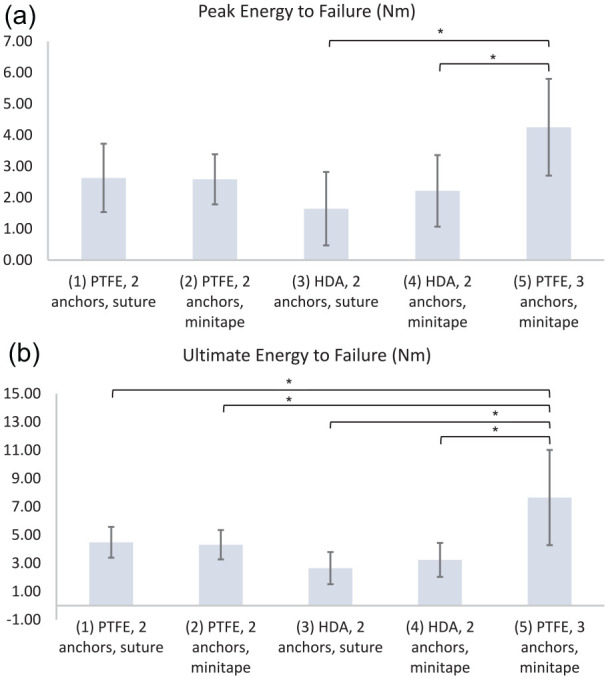
Background: Superior capsule reconstruction (SCR) is an option for the treatment of massive, irreparable rotator cuff tears. However, which materials yield the strongest constructs remains undetermined. Purposes: We sought to investigate whether SCR with polytetrafluoroethylene (PTFE) or human dermal allograft (HDA), 2 or 3 glenoid anchors, and suture or minitape resulted in better failure load properties at the patch-glenoid interface. Methods: We conducted a biomechanical study in 30 glenoid-sided SCR repairs in Sawbones models divided into 5 groups. Each was pulled to failure to assess mode of failure, peak load (N), stiffness (N/mm), yield load (N), peak energy (N m), and ultimate energy (N m). The 5 groups were as follows: group 1-PTFE, 2 anchors, and suture; group 2-PTFE, 2 anchors, and minitape; group 3-HDA, 2 anchors, and suture; group 4-HDA, 2 anchors, and minitape; group 5-PTFE, 3 anchors, and minitape. Results: Repairs failed by button-holing of suture/minitape. Group 5 had greater peak load, stiffness, yield load, and peak energy (384 ± 62 N; 24 ± 3 N/mm; 343 ± 42 N; 4 ± 2 N m) than group 3 (226 ± 67 N; 16 ± 4 N/mm; 194 ± 74 N; 2 ± 1 N m) or group 4 (274 ± 62 N; 17 ± 4 N/mm; 244 ± 50 N; 2 ± 1 N m) and greater ultimate energy (8 ± 3 N m) than all other groups. Conclusions: This biomechanical study of SCR repairs in Sawbones models found that yield load was greater in PTFE than HDA, 3 anchors were better than 2, and minitape was no better than suture.
Keywords: arthroscopy; biomechanics; irreparable rotator cuff tear; superior capsular reconstruction; synthetic.
© The Author(s) 2022.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: George A.C. Murrell, MD, DPhil, reports relationships with Smith & Nephew, the Journal of Shoulder and Elbow Surgery, and Shoulder and Elbow. The other authors declare no potential conflicts of interest.
Figures
References
LinkOut - more resources
Full Text Sources
