

Neutralizing antibodies to Omicron after the fourth SARS-CoV-2 mRNA vaccine dose in immunocompromised patients highlight the need of additional boosters
- PMID: 36776853
- PMCID: PMC9911671
- DOI: 10.3389/fimmu.2023.1104124
Neutralizing antibodies to Omicron after the fourth SARS-CoV-2 mRNA vaccine dose in immunocompromised patients highlight the need of additional boosters
Abstract
Introduction: Immunocompromised patients have been shown to have an impaired immune response to COVID-19 vaccines.
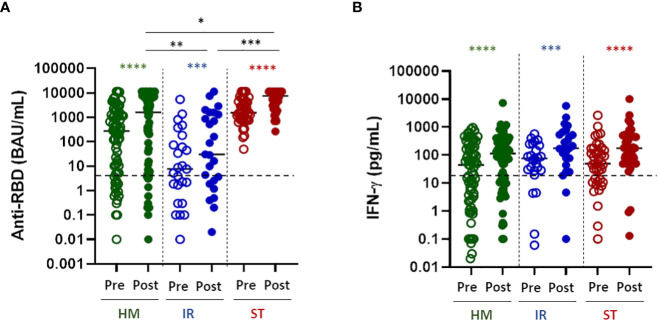
Methods: Here we compared the B-cell, T-cell and neutralizing antibody response to WT and Omicron BA.2 SARS-CoV-2 virus after the fourth dose of mRNA COVID-19 vaccines in patients with hematological malignancies (HM, n=71), solid tumors (ST, n=39) and immune-rheumatological (IR, n=25) diseases. The humoral and T-cell responses to SARS-CoV-2 vaccination were analyzed by quantifying the anti-RBD antibodies, their neutralization activity and the IFN-γ released after spike specific stimulation.
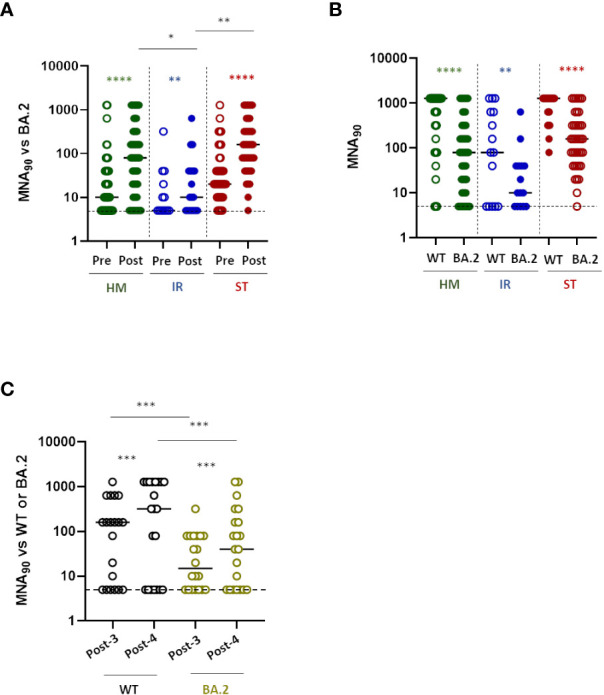
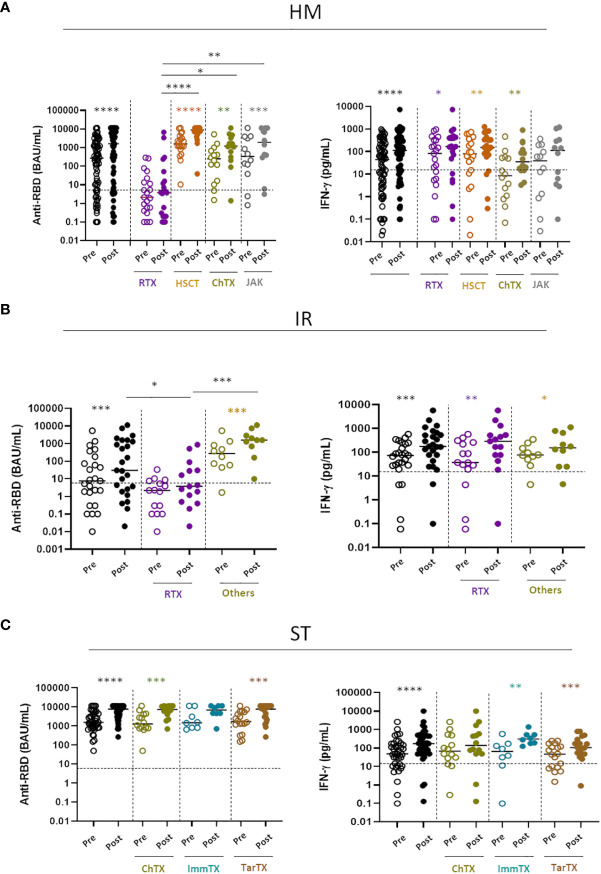
Results: We show that the T-cell response is similarly boosted by the fourth dose across the different subgroups, while the antibody response is improved only in patients not receiving B-cell targeted therapies, independent on the pathology. However, 9% of patients with anti-RBD antibodies did not have neutralizing antibodies to either virus variants, while an additional 5.7% did not have neutralizing antibodies to Omicron BA.2, making these patients particularly vulnerable to SARS-CoV-2 infection. The increment of neutralizing antibodies was very similar towards Omicron BA.2 and WT virus after the third or fourth dose of vaccine, suggesting that there is no preferential skewing towards either virus variant with the booster dose. The only limited step is the amount of antibodies that are elicited after vaccination, thus increasing the probability of developing neutralizing antibodies to both variants of virus.
Discussion: These data support the recommendation of additional booster doses in frail patients to enhance the development of a B-cell response directed against Omicron and/or to enhance the T-cell response in patients treated with anti-CD20.
Keywords: Omicron neutralization; SARS-CoV-2 mRNA vaccine; T cell response; cross immunity; humoral response; immunocompromised patients.
Copyright © 2023 Rescigno, Agrati, Salvarani, Giannarelli, Costantini, Mantovani, Massafra, Zinzani, Morrone, Notari, Matusali, Pinter, Uccelli, Ciliberto, Baldanti, Locatelli, Silvestris, Sinno, Turola, Lupo-Stanghellini, Apolone and the VAX4FRAIL study Group.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Rojas-Botero ML, Fernandez-Nino JA, Arregoces-Castillo L, Ruiz-Gomez F. Estimated number of deaths directly avoided because of COVID-19 vaccination among older adults in Colombia in 2021: An ecological, longitudinal observational study. F1000Res (2022) 11:198. doi: 10.12688/f1000research.109331.2 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous