

Meta-analysis of neoadjuvant immunotherapy for non-metastatic colorectal cancer
- PMID: 36776899
- PMCID: PMC9911889
- DOI: 10.3389/fimmu.2023.1044353
Meta-analysis of neoadjuvant immunotherapy for non-metastatic colorectal cancer
Abstract
Background: Immunotherapy has been approved for the treatment of metastatic colorectal cancer. The efficacy and safety of neoadjuvant immunotherapy for the treatment of non-metastatic colorectal cancer remains unclear. We tried to explore clinical effect of neoadjuvant immunotherapy in the treatment of non-metastatic colorectal cancer.
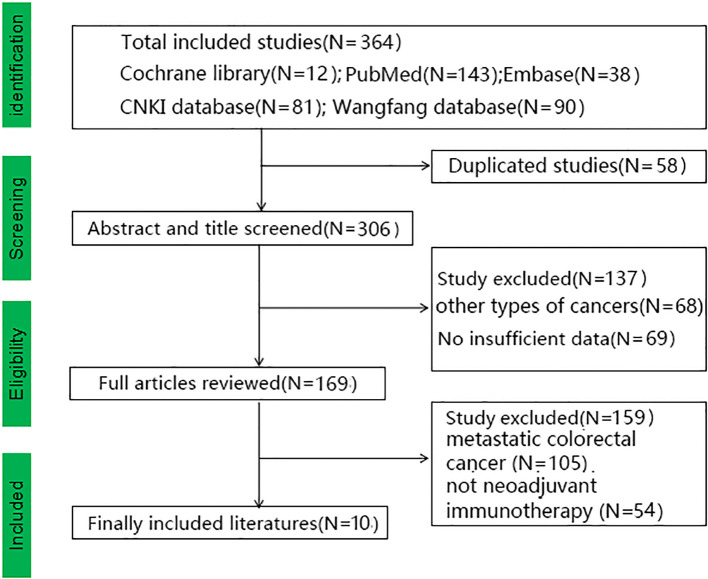
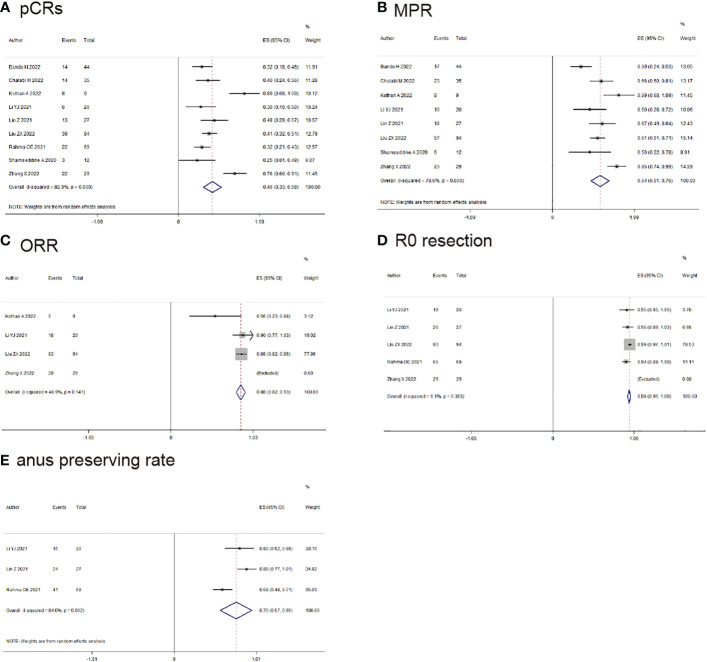
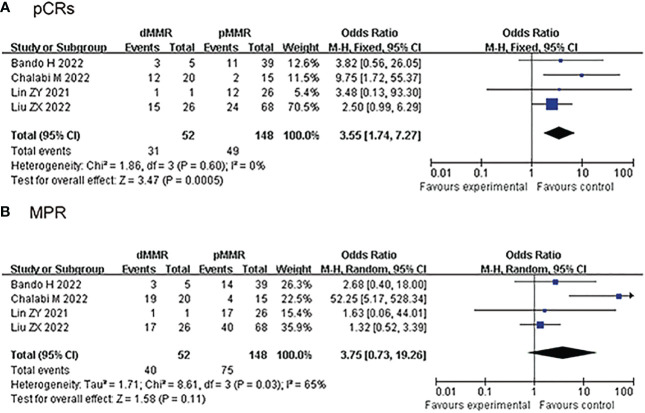
Methods: We searched the databases (PubMed, Wanfang Embase, Cochrane Library and China National Knowledge Infrastructure databases) to obtain suitable articles up to September 2022. The primary outcomes of pathological complete response (pCRs), major pathological response (MPR), objective response rate (ORR), R0-resection and anus preserving rate were collected and evaluated. Secordary outcomes (pCRs and MPR) of subgroup analysis between deficient mismatch repair/microsatellite instability-high group (dMMR/MSI-H) and proficient mismatch repair/microsatellite stable group (pMMR/MSS) and outcomes for rectal cancer were analyzed for the final results.
Results: We included ten articles and 410 cases of non-metastatic colorectal cancer with neoadjuvant immunotherapy. There were 113 (27.5%) cases with the dMMR/MSI-H status and 167 (40.7%) cases with the pMMR/MSS status. pCRs was found in 167/373 (44.6%) patients (ES: 0.49, 95% CI: 0.36 to 0.62, P<0.01, chi2 = 65.3, P<0.01, I 2 = 86.2%) and MPR was found in 194/304 (63.8%) patients (ES: 0.66, 95% CI: 0.54 to 0.78, P<0.01, chi2 = 42.55, P<0.01, I 2 = 81.2%) with the random-effects model and huge heterogeneity. In the subgroup analysis, pCRs was higher in the dMMR/MSI-H group than the pMMR/MSS group in the fixed-effects model with minimal heterogeneity (OR: 3.55, 95% CI: 1.74 to 7.27, P<0.01, chi2 = 1.86, P=0.6, I 2 = 0%). pCRs was found in 58/172 (33.9%) rectal cancer patients (ES: 0.33, 95% CI: 0.26 to 0.40, P<0.01, chi2 = 3.04, P=0.55, I 2 = 0%) with the fixed-effects model and little heterogeneity.
Conclusion: Neoadjuvant immunotherapy could increase pCRs and MPR rate for non-metastatic colorectal cancer. Neoadjuvant immunotherapy could achieve better pCRs rate in dMMR/MSI-H group than in the pMMR/MSS group. Neoadjuvant immunotherapy could be another treatment option for non-metastatic colorectal cancer.
Systematic review registration: https://www.crd.york.ac.uk/prospero/#myprospero, identifier CRD42022350523.
Keywords: dMMR/MSI-H group; meta-analysis; neoadjuvant immunotherapy; non-metastatic colorectal cancer; pMMR/MSS group.
Copyright © 2023 Zhou, Yang, Zhao, Wang and Liu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
The neoadjuvant immunotherapy for non-metastatic mismatch repair-deficient colorectal cancer: a systematic review.Front Immunol. 2025 May 1;16:1540751. doi: 10.3389/fimmu.2025.1540751. eCollection 2025. Front Immunol. 2025. PMID: 40376001 Free PMC article.
-
Neoadjuvant immunotherapy for DNA mismatch repair proficient/microsatellite stable non-metastatic rectal cancer: a systematic review and meta-analysis.Front Immunol. 2025 Jan 27;16:1523455. doi: 10.3389/fimmu.2025.1523455. eCollection 2025. Front Immunol. 2025. PMID: 39931055 Free PMC article.
-
The efficacy and safety of neoadjuvant chemoradiotherapy combined with immunotherapy for locally advanced rectal cancer patients: a systematic review.Front Immunol. 2024 May 15;15:1392499. doi: 10.3389/fimmu.2024.1392499. eCollection 2024. Front Immunol. 2024. PMID: 38846948 Free PMC article.
-
Single-Agent Neoadjuvant Immunotherapy With a PD-1 Antibody in Locally Advanced Mismatch Repair-Deficient or Microsatellite Instability-High Colorectal Cancer.Clin Colorectal Cancer. 2023 Mar;22(1):85-91. doi: 10.1016/j.clcc.2022.11.004. Epub 2022 Nov 25. Clin Colorectal Cancer. 2023. PMID: 36528470
-
[Multicenter real-world study on safety and efficacy of neoadjuvant therapy in combination with immunotherapy for colorectal cancer].Zhonghua Wei Chang Wai Ke Za Zhi. 2022 Mar 25;25(3):219-227. doi: 10.3760/cma.j.cn441530-20220228-00070. Zhonghua Wei Chang Wai Ke Za Zhi. 2022. PMID: 35340171 Chinese.
Cited by
-
Immune checkpoint inhibitors for patients with mismatch repair deficient or microsatellite instability-high advanced cancers: a meta-analysis of phase I-III clinical trials.Int J Surg. 2025 Jan 1;111(1):1357-1372. doi: 10.1097/JS9.0000000000002007. Int J Surg. 2025. PMID: 39166943 Free PMC article.
-
Colorectal Cancer: Risk Factors, Novel Approaches in Molecular Screening and Treatment.Int J Mol Cell Med. 2025;14(1):576-605. doi: 10.22088/IJMCM.BUMS.14.1.576. Int J Mol Cell Med. 2025. PMID: 40123590 Free PMC article. Review.
-
Safety and feasibility of minimally invasive gastrectomy after neoadjuvant immunotherapy for locally advanced gastric cancer: a propensity score-matched analysis in China.Gastroenterol Rep (Oxf). 2024 Feb 28;12:goae005. doi: 10.1093/gastro/goae005. eCollection 2024. Gastroenterol Rep (Oxf). 2024. PMID: 38425656 Free PMC article.
-
Towards the Prediction of Responses to Cancer Immunotherapy: A Multi-Omics Review.Life (Basel). 2025 Feb 12;15(2):283. doi: 10.3390/life15020283. Life (Basel). 2025. PMID: 40003691 Free PMC article. Review.
-
Functional outcomes in rectal cancer patients treated with immunotherapy and neoadjuvant therapy: a retrospective analysis.Langenbecks Arch Surg. 2025 Jun 3;410(1):174. doi: 10.1007/s00423-025-03746-0. Langenbecks Arch Surg. 2025. PMID: 40459755 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical